Abstract: Public first aid measures. Rules of first aid or where to start for a beginner before starting the practice of Banking with potassium permanganate
Every person should know how to provide first aid to those who need it. We are not talking about a full medical understanding of certain complexities associated with various types of diseases.
But for the most common types of symptoms of diseases, injuries, burns and other injuries, you simply need to be able to provide first aid.
Providing first aid
We present to your attention quick guide from the region. With simple instructions and graphic images It will be easy for you to remember how to help someone who is on the verge of life and death.
Of course, after one reading it will be difficult for you to remember all the nuances. After all, first aid has its own specifics.
However, by re-reading this post at least once over a period of time, you can confidently say that you will be a trained rescuer in all the cases described below.
If you are reading this article not for educational purposes, but to benefit from advice in specific circumstances, use the table of contents to quickly jump to the point you need.
First aid
First aid is the only thing you can do to help someone in need. We, as in all textbooks, give standard cases as examples.
An educated individual simply mandatory you need to know these rules.
Bleeding


General questions for bleeding
If a person looks pale, feels chills and feels dizzy, what is it?
This means that he is plunged into a state of shock. Call an ambulance immediately.
Is it possible to get some kind of infection through contact with a patient’s blood?
If possible, it is better to avoid such contacts. It is advisable to use medical gloves, plastic bags, or ask the victim, if possible, to press the wound himself.
Do I need to wash the wound?
You can wash it for minor cuts and abrasions. In case heavy bleeding This should not be done, since washing away the dried blood will only increase the bleeding.
What to do if there is a foreign object inside the wound?
Do not remove it from the wound as this will make the situation worse. Instead, place a tight bandage around the item.
Fractures





Dislocations and sprains
How to determine dislocations or sprains? First, the patient feels pain. Secondly, there is swelling (bruising) around the joint or along the muscle. If a joint is injured, it will be difficult to move.
Provide rest and convince the patient not to move the injured part. Also, don’t try to straighten it yourself.
Apply an ice pack wrapped in a towel to the injured area for no more than 20 minutes.
If necessary, give the victim pain medication.
Go to the emergency room to get an x-ray. If the patient is unable to walk at all or the pain is too severe, call medical help.
First aid for burns
First, cool the burned area under running water. cold water for at least 10 minutes.
Always call medical attention if a child is injured by a burn. Moreover, if the burned area is covered with blisters or internal tissues are visible to the naked eye.
Do not touch anything that is stuck to the burned area. Never lubricate a burn with oil, as it retains heat, and this will only cause harm.
Do not use ice to cool a burn; it can damage the skin.
Airway obstruction


Heart attack
How to detect a heart attack? First of all, it is accompanied pressing pain behind the sternum. Feels like pinpoints discomfort in the arms, neck, jaw, back or stomach.
Breathing becomes frequent and intermittent, and the heartbeat becomes rapid and irregular. In addition, there is a weak and rapid pulse in the extremities, cold and profuse sweat, nausea, and sometimes vomiting.
Call an ambulance immediately, as the minutes are counting. If possible, measure your blood pressure, pulse, and heart rate.
If the patient does not have allergies, give him aspirin. The tablet must be chewed. However, before doing this, make sure that the patient does not have medications prescribed by the attending physician.
Provide the patient with the most comfortable position possible. It is important to reassure and reassure him while waiting for the doctor, since such attacks are sometimes accompanied by a feeling of panic.
Stroke
It is quite easy to identify the symptoms of a stroke. Sudden weakness or numbness in any limb, difficulty speaking and understanding it, dizziness, lack of coordination of movements, sudden headache or fainting - all this indicates a possible stroke.

Place the patient on high pillows, tuck them under the shoulders, shoulder blades and head, and call an ambulance.
Provide air flow in the room fresh air by opening the window. Unbutton your shirt collar, loosen the tight belt, and remove all restrictive clothing. Then measure your blood pressure.
If there are signs of gag reflexes, turn the patient's head to the side. Try to talk calmly and reassure him while waiting for the doctor.
Heatstroke
Heat stroke is determined by the following signs: there is no sweating, body temperature sometimes rises to 40 ° C, hot skin looks pale, blood pressure decreases, and the pulse becomes weak. There may be cramps, vomiting, diarrhea and loss of consciousness.
Move the patient to as cool a place as possible, provide fresh air, and call for medical help.
Remove excess and unfasten tight clothes. Wrap your body in a damp, cool cloth. If this is not possible, place towels soaked in cold water on your head, neck and groin area.
It is advisable for the patient to drink cool mineral or regular, slightly salted water.
If necessary, continue to cool the body by applying ice or cold objects wrapped in a cloth to the wrists, elbows, groin, neck, and armpits.
Hypothermia
As a rule, with hypothermia a person is pale and cold to the touch. He may not be shaking, but his breathing rate is slow and his body temperature is below 35 degrees Celsius.
Call ambulance and move the patient to a warm room, covering him with a blanket. Let him drink a hot drink, but without caffeine or alcohol. The best thing is tea. Offer high-calorie foods.
If you notice signs of frostbite, such as loss of sensation, whitening of the skin or tingling, do not rub the affected areas with snow, oil or petroleum jelly.
This can seriously injure the skin. Just wrap these areas in several layers.
Head injury
For head injuries, the bleeding must first be stopped. Then press a sterile napkin tightly onto the wound and hold it with your fingers until the bleeding stops completely. Next, cold is applied to the head.
Call an ambulance and monitor the presence of pulse, breathing and reaction of the pupils to light. If these signs of life are not present, immediately begin cardiopulmonary resuscitation ().
After breathing and cardiac activity are restored, place the victim in a stable lateral position. Cover and keep him warm.
Drowning
What to do if you see a drowned person? First of all, make sure that you are not in danger and then remove it from the water.
Lay him on his stomach on your knee and let the water naturally drain out of his airway.
Clear your mouth of foreign objects (mucus, vomit, etc.) and call an ambulance immediately.
Determine the presence of a pulse in the carotid artery, the reaction of the pupils to light and spontaneous breathing. If they are not there, start cardiopulmonary resuscitation.
If signs of life appear, turn the person on his side, cover him and keep him warm.
If there is a suspicion of a spinal fracture, the drowned person should be pulled out of the water on a board or shield.
If there is no pulse in the carotid artery, it is unacceptable to waste time removing water from the lungs and stomach.
Get started right away. They must be carried out even if the victim has been under water for more than 20 minutes.
Bites
Insect and snake bites are different, and so is first aid for them.
Insect bites
Carefully inspect the bite site. If you find a sting, carefully pull it out. Then apply ice or a cold compress to the area.
If a person develops an allergy or anaphylactic reaction, call an ambulance.
Snake bites
If a person is bitten by a poisonous snake, call an ambulance immediately. Then inspect the bite site. You can put ice on it.
If possible, keep the affected body part below the heart. Try to calm the person down. Don't let him walk unless absolutely necessary.
Do not under any circumstances cut the bite site or try to suck out the venom yourself.
In case of poisoning snake venom characteristic following signs: nausea, vomiting, tingling sensation in the body, shock, coma or paralysis.
You should know that with any movement of the body, the poison begins to penetrate the tissues of the body much more actively. Therefore, until the doctors arrive, the patient is strongly recommended to rest as much as possible.
Loss of consciousness
What is first aid for loss of consciousness? First of all, don't panic.
Turn the patient on his side to prevent him from choking on possible vomiting. Next, you should tilt his head back so that the tongue moves forward and does not block the airway.
Call an ambulance. Listen to whether the victim is breathing. If not, start CPR.
Cardiopulmonary resuscitation


Artificial respiration
Familiarize yourself with the sequence in which artificial ventilation should be performed.
- Using a circular motion of your fingers wrapped in gauze or a handkerchief, remove mucus, blood, and foreign objects from the victim’s mouth.
- Tilt your head back: lift your chin while maintaining your cervical spine. You should know that if you suspect a fracture cervical spine spine, you cannot throw your head back.
- Pinch the patient's nose with your thumb and index finger. Then do deep breath, and exhale smoothly into the victim’s mouth. Allow 2-3 seconds for passive exhalation of air. Take a new breath. Repeat the procedure every 5-6 seconds.

If you notice that the patient begins to breathe, still continue to blow air along with his inhalation. Continue this until deep spontaneous breathing is restored.
Heart massage
Determine the location of the xiphoid process, as shown in the figure. Determine the point of compression two transverse fingers above the xiphoid process, strictly in the center of the vertical axis. Place the heel of your palm on the compression point.
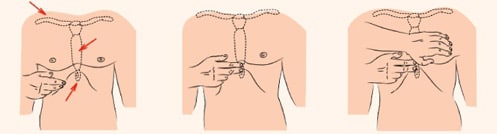 Compression point
Compression point Apply compression strictly vertically along the line connecting the sternum to the spine. Perform the procedure with the weight of the upper half of your body, doing it smoothly, without sudden movements.
The depth of compression of the chest should be at least 3-4 cm. Perform about 80-100 compressions per minute.

Alternate 2 “breaths” of artificial pulmonary ventilation (ALV) with 15 pressures.
For infants, massage is performed using the palmar surfaces of the second and third fingers. For teenagers - with the palm of one hand.
In adults, the emphasis is on the base of the palms, thumb aimed at the head or legs of the victim. The fingers should be raised and not touch the chest.
In the process cardiopulmonary resuscitation monitor for signs of life. This will determine the success resuscitation measures.

First aid– this is extremely important thing in our lives. Nobody knows in what unexpected at the moment these skills can come in handy.
If this article was useful to you, save it on social networks. Use the buttons below to do this.
Who knows, maybe someone who reads this text today will save a person’s life tomorrow.
Do you love and are passionate about personal development? Subscribe to the site website in any convenient way. It's always interesting with us!
Did you like the post? Press any button.
Hello, my dear readers! I looked at my rubrics for a very long time and thought that two of them were sagging in terms of the amount of material. Although it's very useful topics, but somehow their turn doesn’t reach them. I would have continued to think about this topic, and the cart would still be there today, if not for one thing interesting event which happened just yesterday. But more on that later.
I would like to start with the fact that in our life no one is immune from various unpleasant situations and we must be prepared to find a way out of them. Unfortunately, you cannot be prepared for everything; there are simply no such superhumans. But everyone needs to strive to know everything.
I will never forget when, as a child, I needed to provide first aid to my mother - she was bleeding heavily. Unfortunately, at that moment, I did not know what exactly I needed to do, but by some incomprehensible logic I made clear manipulations that allowed me to stop the blood loss.
When at work I tell my students the basic rules of first medical care, they always ask me approximately the same question: “Vladimir Alekseevich, we don’t need this, doctors should do this, we’ll just call an ambulance.” I always have one standard answer prepared for this - and you will watch and wait “ambulance” when an accident happened to a loved one or someone close to you? Of course, in this case everyone will act.
So, what is the main rule for a person who provides first aid to a victim? Do you have any possible answers? I am sure that many have already guessed, but just in case I will point out golden rule PMP:
Do no harm!
That is, by his actions, the person providing assistance should not aggravate the situation; in no case should the victim be caused additional pain or carry out actions that could subsequently affect his health.
And only after a person realizes this principle, not just skims the text or listens to it in a lecture, but precisely when he lets it pass through himself, only after that can he think about studying the techniques of providing primary care.
The second enemy in any critical situation is panic; it is panic that becomes the reason for the illogical and unreasonable actions of any person. In medicine, panic costs life, and, as a rule, someone else's. I have a lot of friends and acquaintances who are doctors, and they periodically tell me different stories. Perhaps, let me tell you a couple of them.
Several years ago I came across a very savvy lecturer on first aid and she told me the following story. I’ll make a reservation right away - the person worked in an ambulance, so he’s seen a lot and it’s difficult to cast doubt on her story.
So, imagine a Moscow beach, our people are having a cultural holiday - swimming in a pond, sunbathing on the shore, drinking, eating, and generally not doing anything unusual. And towards evening, our compatriot, who had fallen asleep on the beach and was slightly overindulgent, discovered that his tongue was pinned to his cheek. Pin to cheek! Can you imagine? The doctors could only guess what happened.
As a result, the main version is this: seeing a person unconscious, a conscientious citizen provided first aid to the victim - performed a rescue turn (turned the “victim” on his side) and pinned his tongue to his cheek so that the person who had had too much would not swallow his tongue. From the point of view of first aid, everything was correct: they turned him on his side so that he would not choke on vomit and prevented his tongue from sticking into the respiratory tract. But how harsh!
First aid with improvised materials
Imagine: a factory, a work shift, everyone is minding their own business, suddenly one of the workers falls on the floor right in the workshop and begins to convulse - he has an epileptic attack.
Naturally, his colleagues helped him as best they could: again, it is necessary to prevent injury to the victim and prevent the tongue from sticking. Well, to immobilize him is simple - they piled on with their entire strike team and pressed his body to the floor, but how to unclench his jaws? After all, with such convulsions, it’s not difficult to bite off your tongue.
They opened it with whatever came to hand... a screwdriver. The result is that 8 teeth are broken, but the tongue is still there. I don’t think that the victim, when he came to his senses, thanked his colleagues.
I myself, in line at the store, witnessed a similar situation - a man felt ill, there was no spoon at hand and our good citizens wanted to unclench their jaws with a bottle opener, a corkscrew and everything that was very close to the cash register. Thank God they didn't succeed.
What prompted me to write this article
Today I was lucky enough to visit the Russian National Research medical university named after N.I. Pirogov. In principle, an ordinary event that had nothing to do with first aid, but for some reason it was this that prompted me to write this post. I just looked at these desperate, intelligent people who want to devote themselves to medicine, i.e. helping people.
Our acquaintance with the university began at the Department of Dental Therapy. It was very interesting to see how dentists are trained. Friends, those who say that dentists are not doctors know nothing about dentistry. Future dentists are taught almost everything that other doctors are taught, including anatomy.
And looking at the teachers, I will tell you that studying there is no easier than in the surgical department, for example. I’ll add a couple of photos of a phantom office - this is an office in which students work using special equipment.

Then we visited the university museum - we learned the story of Pirogov - he was an outstanding doctor, I’ll tell you, I never knew that he was the first to use ether (gas) anesthesia, created an anatomical atlas internal organs man and made many, many more useful discoveries and did many good deeds. And here is the office of the zemstvo doctor, just to understand what they were like:

And this is an innovative office for surgeons: on this simulator, future surgeons hone their skills. Imagine: a simulator on which you can practice any operation - the children in the photo are removing gallbladder: 
Many people criticize our medicine, but in fact it is one of the best in the world. And our doctors are highly valued abroad, as they undergo very high-quality training.
At the end of my article, I want to announce to you the release of a number of articles on first aid on my blog. By the end of the year, I will try to write and publish a number of articles on the rules of PMP. I sincerely hope that this knowledge will never be useful to you in your life. I will end here, subscribe to blog updates so as not to miss the release of new articles, share the information from this post with your friends on social networks. Until we meet again, bye-bye!
Introduction
- The history of the origins of first medical aid___________________________
- Rules and principles of first aid.__________________
3. Practical Application publicly available first aid measures._______________________________________________________________
3.1 Cardiopulmonary failure._________________________________
3.1.1 Artificial ventilation using the “donor” method.______________
3.1.2 Indirect cardiac massage._____________________________________________
3.2 Bruises, sprains, fractures._____________________________________________
3.3 Injuries.__________________________________________________________
3.4 Drowning.________________________________________________________________
3.5 Burns.__________________________________________________________
3.6 Frostbite.__________________________________________________________
3.7 Electric shock.)__________________________________________
3.8 Heat (sunstroke) _____________________________________________
4. Transportation of victims. ___________________________________________
Conclusion__________________________________________________________________
List of used literature________________________________________________
Introduction
Know for sure - Act correctly - Save lives!
First aid is the simplest expedient measures to save the health and life of a person who has suffered an injury.
Correctly applied first aid measures reduce the time of special treatment, promotes faster healing wounds and is often the decisive moment in saving the life of the victim. First aid should be provided immediately at the scene of the accident quickly and skillfully even before the arrival of the doctor or before transporting the victim to the hospital.
The essence of first aid is to stop further exposure to traumatic factors, carry out simple measures and ensure prompt transportation of the victim to a medical facility. Its task is to prevent dangerous consequences trauma, bleeding, infection and shock.
First aid is a set of simple, expedient measures to protect the health and life of a person who has suffered an injury or suddenly fallen ill.
The work examines in detail publicly available first aid measures. Since just knowledge of first aid measures does not allow us to provide the entire range of measures to save the life and health of the victim, the work examines generally available first aid measures in relation to the causes of situations that are harmful to human life and health.
1. History of first aid .
Providing first aid is a natural part of our lives. Its origin dates back to the early dawn of humanity.
First aid is mentioned in records on Egyptian papyri, in poems by Greek poets, in the works of ancient Roman writers and in biblical legends. Naturally, in the Ancient World and the Middle Ages, the level of first aid corresponded to the level of medicine of that time. Knowledge of structure human body prevented by prejudices about the inviolability of corpses. The progressive development of medicine began only in modern times, when, thanks to the famous 16th century physician Vessalius, medical knowledge enriched and became more accurate. At that time they appear scientific justification first aid measures, new, more improved ways of providing it arise. This was also facilitated by the discovery English doctor Lister of the last century, who proved the need for sterility in the treatment of wounds and operations. Purity was achieved through antiseptics- a method of combating pathogenic germs, which consists of washing the hands of the surgeon and the surgical field, as well as sterilizing operating instruments. The greatest merit in organizing first aid in the last century belongs to the Russian surgeon Pirogov, who in 1853, during the Crimean War, introduced targeted treatment of wounds in the field.
The importance of first aid and its tasks are great not only during war; the role of first aid is no less important in peacetime in protecting human health and in improving the health of their living environment.
2. Rules and principles of first aid.
When providing first aid, it is necessary to adhere to a certain sequence, which requires a quick and correct assessment of the victim’s condition.
First you need to imagine the circumstances under which the injury occurred and which influenced its occurrence and nature.
Need to install:
1) the circumstances under which the injury occurred;
2) time of injury;
3) the location of the injury.
During inspection it is necessary to establish:
1) type and severity of injury;
2) processing method;
3) necessary first aid equipment depending on the given capabilities and circumstances.
In severe cases (arterial bleeding, unconsciousness, suffocation), first aid must be provided immediately. If the person providing assistance does not have the necessary funds at his disposal, then someone else called to help should help him find them.
Principles of first aid:
1) correctness and appropriateness;
2) speed;
3) thoughtfulness, determination and calmness.
3. Practical application of publicly available first aid measures:
3.1 Cardiopulmonary failure;
Modern methods of reviving sick and injured people are based on the fact that they have three advantages over other previously used methods based on changing the volume of the chest, namely:
In the exhaled air of the “donor” the oxygen content reaches 17%, sufficient for absorption by the victim’s lungs;
Exhaled air contains carbon dioxide- up to 4%.
Compared to other techniques, it provides a larger volume of air entering the victim’s lungs.
To do this you should:
 1. Give the patient the appropriate position: lay him on a hard surface, placing a cushion of clothing under his shoulder blades on his back. Throw your head back as much as possible.
1. Give the patient the appropriate position: lay him on a hard surface, placing a cushion of clothing under his shoulder blades on his back. Throw your head back as much as possible.
2. Open your mouth and look around oral cavity. With convulsive compression masticatory muscles To open it, use a knife, screwdriver, spoon, etc. Clear the oral cavity of mucus and vomit with a handkerchief wrapped around your index finger.
3. Get up with right side. With your left hand, holding the victim’s head in an tilted position, at the same time cover the nasal passages with your fingers. The right hand should be pushed forward and upward lower jaw. The following manipulation is very important:
a) hold the jaw by the zygomatic arches with the thumb and middle finger;
b) open the oral cavity slightly with the index finger;
c) tips ring finger and the little finger (4th and 5th fingers) control the pulse beat in the carotid artery.
4.Take a deep breath, wrap your lips around the victim’s mouth and inhale. Cover your mouth with any clean cloth beforehand for hygienic purposes.
At the moment of inflation, use your eyes to control the rise of the chest.
The frequency of respiratory cycles is 12-15 per minute.
When signs of spontaneous breathing appear in the victim, mechanical ventilation is not stopped immediately, continuing until then. until the number of spontaneous breaths corresponds to 12-15 per minute.
3.1.2 Indirect cardiac massage.
 Heart massage- mechanical impact on the heart after it stops in order to restore its activity and maintain continuous blood flow until the heart resumes functioning. Indications for cardiac massage are all cases of cardiac arrest. The heart may stop beating various reasons: spasm coronary vessels, acute heart failure, myocardial infarction, severe trauma, lightning or electric shock, etc. Signs sudden stop hearts- severe pallor, loss of consciousness, disappearance of the pulse in the carotid arteries, cessation of breathing or the appearance of rare, convulsive breaths, dilation of the pupils.
Heart massage- mechanical impact on the heart after it stops in order to restore its activity and maintain continuous blood flow until the heart resumes functioning. Indications for cardiac massage are all cases of cardiac arrest. The heart may stop beating various reasons: spasm coronary vessels, acute heart failure, myocardial infarction, severe trauma, lightning or electric shock, etc. Signs sudden stop hearts- severe pallor, loss of consciousness, disappearance of the pulse in the carotid arteries, cessation of breathing or the appearance of rare, convulsive breaths, dilation of the pupils.
 There are two main types of cardiac massage: indirect, or external (closed), and direct, or internal (open).
There are two main types of cardiac massage: indirect, or external (closed), and direct, or internal (open).
Indirect cardiac massage is based on the fact that when pressing on the chest from front to back, the heart, located between the sternum and the spine, is compressed so much that blood from its cavities enters the vessels. After the pressure stops, the heart straightens and venous blood enters its cavity.
Circulatory efficiency created by cardiac massage, determined by three criteria: occurrence of pulsation carotid arteries in time with the massage, constriction of the pupils and the appearance of independent breaths. The effectiveness of chest compressions
is ensured by the correct choice of the place where force is applied to the victim’s chest (the lower half of the sternum immediately above the xiphoid process). The massager’s hands must be correctly positioned (the proximal part of the palm of one hand is placed on the lower half of the sternum, and the palm of the other is placed on the back of the first, perpendicular to its axis; the fingers of the first hand should be slightly raised and not put pressure on the victim’s chest).
They should be straight at the elbow joints. The person performing the massage should stand quite high (sometimes on a chair, stool, stand, if the patient is lying on a high bed or on the operating table), as if hanging his body over the victim and putting pressure on the sternum not only with the force of his hands, but also with the weight of his body. The pressing force should be sufficient to move the sternum towards the spine by 4-6 cm. The pace of the massage should be such as to provide at least 60 heart compressions per minute. When performing resuscitation by two persons, the massager compresses the chest 5 times with a frequency of approximately 1 time per 1 second, after which the second person providing assistance makes one vigorous and quick exhalation from the mouth to the mouth or nose of the victim. 12 such cycles are carried out in 1 minute. If resuscitation is carried out by one person, then the specified mode of resuscitation measures becomes impossible; the resuscitator is forced to perform chest compressions at a more frequent rhythm - approximately 15 heart compressions in 12 seconds, then 2 vigorous blows of air into the lungs in 3 seconds; 4 such cycles are performed in 1 minute, resulting in 60 heart compressions and 8 breaths.
3.2 Bruises, sprains, fractures.
Injury– closed damage to tissues and organs without significant disruption of their structure. Typically caused by blunt force trauma or a fall. Superficially located tissues (skin, subcutaneous tissue, muscles and periosteum) are more often damaged.
At first aid for victims with bruises, if there is even the slightest suspicion of a more severe injury (fracture, dislocation, damage to internal organs, etc.), its volume must correspond to the severity of the alleged injury. If breathing or cardiac function is impaired, they immediately begin at the scene of the incident. artificial respiration and cardiac massage. At the same time, an ambulance is called.
Helps reduce pain from minor soft tissue bruises local application cold: direct a stream of cold water to the damaged area, apply a bubble or heating pad with ice to it, or make cold lotions. It is recommended that immediately after an injury, apply a pressure bandage to the site of the bruise and create rest; for example, if a hand is bruised, its rest can be ensured with the help of a scarf bandage. If the leg is bruised, it is given an elevated position, a gentle load regime is observed for several days, and then, as the pain and swelling decrease, it is gradually expanded.
 Sprains and tears of ligaments, tendons, muscles are among the most common injuries of the musculoskeletal system. A characteristic feature tearing or spraining is a violation motor function a joint that is strengthened by the corresponding ligament, or a muscle if it itself or its tendon is damaged.
Sprains and tears of ligaments, tendons, muscles are among the most common injuries of the musculoskeletal system. A characteristic feature tearing or spraining is a violation motor function a joint that is strengthened by the corresponding ligament, or a muscle if it itself or its tendon is damaged.
The main measures for sprains and ruptures of ligaments are to provide rest to the damaged joint, apply a tight bandage and, to reduce pain, apply a cold compress for 12-24 hours, then switch to heat and warming compresses.
 Dislocation– persistent displacement of the articular ends of the bones, which causes dysfunction of the joint.
Dislocation– persistent displacement of the articular ends of the bones, which causes dysfunction of the joint.
When applying first aid measures to the victim at the scene of the accident, you should not try to reduce the dislocation, because this often causes additional injury. It is necessary to provide rest to the damaged joint by immobilizing it. It is necessary to apply cold to it (ice pack or cold water). In case of open dislocation, a sterile bandage is first applied to the wound. Warming compresses should not be used. The doctor must correct the dislocation within the first hours after the injury.
Fractures– damage to bones, which are accompanied by a violation of its integrity. In case of fractures, along with damage to the bone, the integrity of the surrounding soft tissues is disrupted, nearby muscles, blood vessels, nerves, etc. can be injured. If the fracture is accompanied by damage to the skin and the presence of a wound, the fracture is called open, and if the skin is intact, it is called closed.
 When providing first aid, you should never try to match bone fragments - to eliminate a change in the shape of the limb (curvature) in the case of a closed fracture, or to set the protruding bone in case of
When providing first aid, you should never try to match bone fragments - to eliminate a change in the shape of the limb (curvature) in the case of a closed fracture, or to set the protruding bone in case of
open fracture.
The victim must be taken to a medical facility as quickly as possible. It is first necessary to ensure reliable transport immobilization, and in case of an open fracture, also apply a sterile bandage to the wound. In case of severe bleeding, it is necessary to take measures to stop it, for example, using a hemostatic tourniquet.
3.3 Drowning;
Drowning- death from hypoxia, which occurs as a result of the closure of the respiratory tract with liquid, most often water. A drowned person can be saved if first aid is provided promptly and correctly.
In the first minute after drowning in water, more than 90% of victims can be saved, after 6-7 minutes - only about 1-3%.
Conventionally, there are several main types of drowning - true, dry and so-called syncope. In the first case, water fills the airways and lungs, the drowning person, fighting for his life, makes convulsive movements and draws in water, which prevents the flow of air. The skin of a drowned person is bluish, and foamy liquid is released from the mouth and nose. In the second case (with dry drowning), due to spasm of the vocal cords, water does not enter the lungs (hence the name), the bluishness of the skin is less pronounced. This type of drowning is accompanied by fainting, and the drowned person immediately sinks to the bottom. In the third case (syncope drowning), the cause of death of the victim is a sudden cessation of breathing and cardiac arrest. Such drowned people have pale skin (the so-called pale drowned).
First aid measures for a drowning person.
If the victim is conscious, has a satisfactory pulse and is breathing, then it is enough to lay him on a dry hard surface so that his head is low, then undress him, rub him with his hands or a dry towel. It is advisable to give a hot drink (tea, coffee, adults can have a little alcohol, for example 1-2 tablespoons of vodka), wrap them in a warm blanket and let them rest.
If the victim is unconscious when removed from the water, but has a satisfactory pulse and breathing, then you should throw back his head and extend his lower jaw, then lay him down so that his head is low, then with your finger (preferably wrapped in a handkerchief) free his oral cavity from silt, mud and vomit, wipe him dry and warm him. A victim who is unconscious, does not breathe independently, but retains cardiac activity, after preliminary measures aimed at clearing the airways, artificial respiration must be started as quickly as possible. If the victim has no breathing or cardiac activity, artificial respiration must be combined with cardiac massage.
 First, as quickly as possible, fluid should be removed from the respiratory tract (in case of drowning in fresh water, only the mouth and throat should be cleared of it). For this purpose, the person providing assistance places the victim with his stomach on the thigh of the leg bent at the knee joint, presses his hand on the victim’s back between the shoulder blades, while supporting his forehead with the other hand and raising his head. You can tilt the victim over the side of a boat, or, placing him face down, lift him in the pelvic area. These manipulations should not take more than 10-15 seconds so as not to delay artificial respiration.
First, as quickly as possible, fluid should be removed from the respiratory tract (in case of drowning in fresh water, only the mouth and throat should be cleared of it). For this purpose, the person providing assistance places the victim with his stomach on the thigh of the leg bent at the knee joint, presses his hand on the victim’s back between the shoulder blades, while supporting his forehead with the other hand and raising his head. You can tilt the victim over the side of a boat, or, placing him face down, lift him in the pelvic area. These manipulations should not take more than 10-15 seconds so as not to delay artificial respiration.
3.5 Injuries.
Wounds– tissue damage caused by mechanical stress, accompanied by damage to the integrity of the skin or mucous membranes. Depending on the mechanism of injury and the nature of the wounding object, cut, stab, chopped, bitten, bruised, gunshot and other wounds are distinguished.
With small, superficial wounds, bleeding is usually capillary, stopping on its own or after applying a pressure bandage. If damaged large vessels bleeding is intense and can threaten the life of the victim.
In the human body, 70% of the total volume of circulating blood is found in the venous bed, 12% in capillaries, 3% in the vessels and chambers of the heart, and only 15% of the circulating blood volume in the arterial bed.
Depending on which vessel is bleeding, bleeding can be capillary, venous, mixed and arterial. With external capillary bleeding, blood is released evenly from the entire wound (like from a sponge); with venous it flows out in a uniform stream, has a dark cherry color (in case of damage large vein There may be a pulsation of the blood stream in rhythm with breathing). During arterial bleeding, the flowing blood has a bright red color, it flows in a strong intermittent stream (fountain), the blood ejects correspond to the rhythm of heart contractions. Mixed bleeding has signs like:
arterial and venous. Bleeding through the mouth may be associated with bleeding from the lungs, upper respiratory tract, pharynx, esophagus and stomach.
First aid measures for external bleeding depends on  his character. So, with a small capillary or venous bleeding from a wound on the arm or leg, it is enough to apply a sterile bandage and bandage it tightly (pressure bandage) or firmly tighten a cotton-gauze swab to the wound using an adhesive plaster. The bandage should consist of several layers of cotton wool and gauze. You need to be careful not to tighten the limb too much (until the skin below the bandage turns blue). Pressure bandage helps stop bleeding from small arteries. Before applying an aseptic dressing, the skin around the wound is freed from clothing and treated with a 2% solution of brilliant green or 5% alcohol solution Yoda. The wound can be washed with a solution of hydrogen peroxide.
his character. So, with a small capillary or venous bleeding from a wound on the arm or leg, it is enough to apply a sterile bandage and bandage it tightly (pressure bandage) or firmly tighten a cotton-gauze swab to the wound using an adhesive plaster. The bandage should consist of several layers of cotton wool and gauze. You need to be careful not to tighten the limb too much (until the skin below the bandage turns blue). Pressure bandage helps stop bleeding from small arteries. Before applying an aseptic dressing, the skin around the wound is freed from clothing and treated with a 2% solution of brilliant green or 5% alcohol solution Yoda. The wound can be washed with a solution of hydrogen peroxide.
In case of severe arterial or mixed bleeding, these first aid measures are not enough. The most accessible of them is to press the artery above the wound from which the blood is flowing. To do this, you need to know the points at which the arteries can be pressed against the bone. As a rule, it is possible to feel the pulsation of the arteries in them. Pressing the artery with a finger or fist provides almost immediate bleeding stop. However, even very good physically developed person cannot continue pressing for long enough, because within 10-15 minutes, the hands begin to get tired and the pressure weakens. In this regard, immediately after pressing the artery, an attempt should be made to stop the bleeding in another way. More often a tourniquet is used for this purpose. After applying a tourniquet, the bleeding should stop, but if it continues, then the tourniquet must be removed and applied again, retreating above the place where it was initially applied. After applying the tourniquet, securely attach a note to it indicating the time, date of application, name and position of the rescuer.
 A tourniquet should be applied in case of severe arterial bleeding above the wound site on the upper third of the shoulder, on all parts of the thigh. The pressure on the limb should be sufficient to stop bleeding, but not cause complete bleeding of the limb. The tourniquet can be applied to the limb for no more than 1.5 - 2 hours, and in the cold season - 0.5 - 1 hour. Periodically, after 30 - 60 minutes, the tourniquet should be loosened, released for a few minutes (during this time, clamp the vessel above the tourniquet with your finger), massage (lightly) the groove from the tourniquet, having previously resumed finger pressure on the artery, and apply again, but with greater tension. If there is no factory-made harness, it can be replaced with an improvised one - a rubber tube, a tie, a belt, a belt, a scarf, a bandage, etc., but you should not use wire. To stop bleeding using improvised means, use the so-called twist, which is then fixed with a separate bandage.
A tourniquet should be applied in case of severe arterial bleeding above the wound site on the upper third of the shoulder, on all parts of the thigh. The pressure on the limb should be sufficient to stop bleeding, but not cause complete bleeding of the limb. The tourniquet can be applied to the limb for no more than 1.5 - 2 hours, and in the cold season - 0.5 - 1 hour. Periodically, after 30 - 60 minutes, the tourniquet should be loosened, released for a few minutes (during this time, clamp the vessel above the tourniquet with your finger), massage (lightly) the groove from the tourniquet, having previously resumed finger pressure on the artery, and apply again, but with greater tension. If there is no factory-made harness, it can be replaced with an improvised one - a rubber tube, a tie, a belt, a belt, a scarf, a bandage, etc., but you should not use wire. To stop bleeding using improvised means, use the so-called twist, which is then fixed with a separate bandage.
 Stopping bleeding from the vessels of the extremities is possible with forced flexion. More often this method is used to stop bleeding from the vessels of the arm. It is rational to use it for intense bleeding from wounds located at the base of the limbs. Maximum flexion of the limb is performed in the joint above the wound and the limb is fixed with bandages in this position. So, when stopping bleeding from wounds of the forearm and hand, a cotton-gauze pad is placed on the flexor surface of the elbow joint (it can be replaced with a small cloth roller), then the arm is bent as much as possible at the elbow, pulling the forearm to the shoulder with a bandage or belt until the pulse disappears. wrist, stopping the flow of blood from the wound. In this position, the hand is fixed with a bandage (belt). In case of bleeding from the upper part of the shoulder and subclavian region, which can be fatal, both shoulders are brought behind the back with elbow joints bent, after which they are tied with a bandage (belt, etc.). In this case, the arteries on both sides are compressed.
Stopping bleeding from the vessels of the extremities is possible with forced flexion. More often this method is used to stop bleeding from the vessels of the arm. It is rational to use it for intense bleeding from wounds located at the base of the limbs. Maximum flexion of the limb is performed in the joint above the wound and the limb is fixed with bandages in this position. So, when stopping bleeding from wounds of the forearm and hand, a cotton-gauze pad is placed on the flexor surface of the elbow joint (it can be replaced with a small cloth roller), then the arm is bent as much as possible at the elbow, pulling the forearm to the shoulder with a bandage or belt until the pulse disappears. wrist, stopping the flow of blood from the wound. In this position, the hand is fixed with a bandage (belt). In case of bleeding from the upper part of the shoulder and subclavian region, which can be fatal, both shoulders are brought behind the back with elbow joints bent, after which they are tied with a bandage (belt, etc.). In this case, the arteries on both sides are compressed.
In case of any bleeding, the injured part of the body is given an elevated position and rest is ensured (transport immobilization).
3.6 Burns
Burns– tissue damage caused by exposure high temperature, electric current, acids, alkalis or ionizing radiation. Accordingly, thermal, electrical, chemical and radiation burns are distinguished. Thermal burns are the most common, accounting for 90-95% of all burns.
The severity of burns is determined by the area and depth of tissue damage. Depending on the depth of the injury, four degrees of burns are distinguished. Superficial burns (I, II degrees) with favorable conditions heal on their own. Deep burns (III and IV degrees) affect, in addition to the skin, deep-lying tissues, so such burns require skin transplantation. Most victims usually have a combination of burns of varying degrees.
Inhalation of flame, hot air and steam can cause burns to the upper respiratory tract and swelling of the larynx with the development of breathing problems. Inhaled smoke may contain nitric or nitrous acids, and when burning plastic, phosgene and gaseous hydrocyanic acid. This smoke is poisonous and causes chemical burns and pulmonary edema. In case of fires in enclosed spaces, lung damage should always be suspected in victims. Burns of the upper respiratory tract and damage to the lungs lead to disruption of oxygen delivery to the body tissues (hypoxia). In adults, hypoxia is manifested by anxiety, pale skin, in children - severe fear, tearfulness, and sometimes spastic muscle contractions and convulsions occur. Hypoxia is the cause of many deaths in indoor fires.
First aid consists of stopping the effect of the damaging factor. In case of flame burns, you should extinguish burning clothing and remove the victim from the fire zone; In case of burns from hot liquids or molten metal, quickly remove clothing from the burn area. To stop the effects of the temperature factor, rapid cooling of the affected area of the body is necessary by immersion in cold water, under running cold water, or irrigation with chlorethyl. At chemical burns(except for burns with quicklime), the affected surface is washed with plenty of tap water as quickly as possible. In case of chemical impregnation active substance Clothes should be removed quickly. Any manipulations on the burn wounds. For the purpose of pain relief, the victim is given analgin (pentalgin, tempalgin, sedalgin). For large burns, the victim takes 2-3 tablets acetylsalicylic acid(aspirin) and 1 tablet of diphenhydramine. Before the doctor arrives, they give you hot tea and coffee, alkaline mineral water (500-2000 ml) or the following solutions: I solution – sodium bicarbonate (baking soda) 1/2 teaspoon. l., sodium chloride (table salt) 1 teaspoon. l. for 1 liter of water; II solution – tea, to 1 liter of which add 1 teaspoon. l. table salt and 2/3 teaspoon. l. sodium bicarbonate or sodium citrate. On burnt surfaces after treatment 70% ethyl alcohol or apply aseptic dressings with vodka. For extensive burns, the victim is wrapped in a clean cloth or sheet and immediately taken to the hospital.
Application to the burn surface immediately after the burn various ointments or fish oil are not justified, because they heavily contaminate the wound, making it difficult to further treat it and determine the depth of the lesion.
3.7 Frostbite.
Frostbite– tissue damage due to exposure to low temperatures. The causes of frostbite are different, and under appropriate conditions (prolonged exposure to cold, wind, high humidity, tight or wet shoes, stationary position, poor general condition victim - illness, exhaustion, alcohol intoxication, blood loss, etc.) frostbite can occur even at a temperature of plus 3-7.
More susceptible to frostbite distal sections limbs, ears, nose. With frostbite, a feeling of cold is initially felt, followed by numbness, during which pain first disappears, and then all sensitivity. The onset of anesthesia makes the ongoing effects of low temperature invisible, which most often causes severe irreversible changes in tissues.
There are four degrees of frostbite based on severity and depth. This can only be determined after the victim has warmed up, sometimes after several days.
Frostbite of the first degree is characterized by skin damage in the form of reversible circulatory disorders. The victim's skin is pale in color, somewhat swollen, its sensitivity is sharply reduced or completely absent. After warming, the skin acquires a blue-purple color, swelling increases, and dull pain. Inflammation (swelling, redness, pain) lasts for several days, then gradually goes away. Later, peeling and itching of the skin occurs. The frostbitten area often remains very sensitive to cold.
Frostbite of the second degree is manifested by necrosis of the superficial layers of the skin. When warmed up, the pale skin of the victim acquires a purplish-blue color, and tissue swelling quickly develops, spreading beyond the frostbite. In the frostbite zone, blisters filled with clear or white liquid form. Blood circulation in the area of damage is restored slowly. Impairment of skin sensitivity may persist for a long time, but at the same time significant pain is noted.
This degree of frostbite is characterized by general phenomena: increased body temperature, chills, poor appetite and sleep. If a secondary infection does not occur, a gradual rejection of dead skin layers occurs in the damaged area without the development of granulation and scars (15-30 days). The skin in this area remains bluish for a long time, with reduced sensitivity.
With third degree frostbite, a violation of the blood supply (vascular thrombosis) leads to necrosis of all layers of skin and soft tissue to varying depths. The depth of damage is revealed gradually. In the first days, skin necrosis is observed: blisters appear filled with dark red and dark brown liquid. An inflammatory shaft (demarcation line) develops around the dead area. Damage to deep tissues is detected after 3-5 days in the form of developing wet gangrene. The tissues are completely insensitive, but patients suffer from excruciating pain.
IV degree frostbite is characterized by necrosis of all layers of tissue, including bone. At this depth of damage, it is not possible to warm up the damaged part of the body; it remains cold and completely insensitive. The skin quickly becomes covered with blisters filled with black liquid. The damage boundary is revealed slowly. A clear demarcation line appears after 10-17 days. The damaged area quickly turns black and begins to dry out (mummify). The process of rejection of a necrotic limb is long (1.5-2 months), wound healing is very slow and sluggish.
In case of frostbite of the first degree and limited areas of the body (nose, ears), warming can be carried out using the warmth of the first aid provider’s hands and heating pads. You should refrain from intensive rubbing and massage of the cooled part of the body, because... with frostbite of degrees II, III and IV, this can lead to injury to blood vessels, which will increase the risk of thrombosis and thereby increase the depth of tissue damage.
Great value at application of first aid measures have measures to generally warm the victim (hot coffee, tea, milk). Fastest delivery bringing the victim to a medical facility is also a first aid measure. During transportation, all measures should be taken to prevent re-cooling. If first aid was not provided before the arrival of the ambulance, it should be provided during transportation.
The main thing is to prevent warming of hypothermic areas of the body from the outside, because Warm air, warm water, the touch of warm objects and even hands have a detrimental effect on them.
When the victim is brought into a heated room, the hypothermic areas of the body, usually the arms or legs, must be protected from the effects of heat by applying thermal insulation to them. dressings (cotton-gauze, wool and others).
The bandage should cover only the area with the affected blanching of the skin, without covering the unchanged skin. Otherwise, heat from areas of the body with unimpaired blood circulation will spread under the bandage to overcooled areas and cause them to warm up from the surface, which cannot be allowed.
The bandage is left in place until a feeling of heat appears and sensitivity in the fingers or toes is restored. In this case, tissue warming will occur due to the heat brought by the blood flow and the vital activity of the tissues of the affected area will be restored simultaneously with the restoration of blood flow in it.
It is very important to ensure the immobility of hypothermic fingers and toes, since their vessels are very fragile and therefore hemorrhages are possible after blood flow is restored. To ensure their immobility, it is enough to use any of the types transport immobilization improvised or standard tires.
In case of general hypothermia with loss of consciousness, the main rule remains the imposition of heat-insulating bandages on the arms and legs as soon as the victim was brought into a warm room. Previously, signs of life are determined in him in the form of the presence of elements of consciousness, breathing, heartbeat, and the reaction of the pupils to light. The body is wrapped in a cotton or wool blanket. The frozen shoes are not removed and the feet in these shoes are wrapped in any available material.
After rendering necessary assistance The victim’s condition is monitored and subsequently hospitalized in a medical facility.
Using this first aid method, it is often possible to save frostbite victims and avoid severe consequences frostbite of hands and feet.
3.8 Electric shock.
Electrical injury– damage resulting from exposure to electric current great strength or a discharge of atmospheric electricity (lightning).
Electrical injury occurs not only during direct contact of the human body with a current source, but also during arc contact when a person is close to an installation with a voltage of more than 1000 V, especially in rooms with high air humidity.
Electric current causes local and general disorders in the body. Local changes are manifested by tissue burns at the places where the electric current exits and enters. Depending on the condition of the affected person (wet skin, fatigue, exhaustion, etc.), the strength and voltage of the current, different local manifestations– from loss of sensitivity to deep burns. When exposed to an alternating current of 15 mA, the victim experiences convulsions (the so-called non-releasing current). In case of electric shock with a force of 25-50 mA, breathing stops. Due to spasm of the vocal cords, the victim cannot scream and call for help. If the effect of the current does not stop, within a few minutes cardiac arrest occurs as a result of hypoxia and the death of the victim occurs. The condition of the victim at the time of electrical injury can be so severe that he is outwardly not much different from the deceased: pale skin, wide pupils that do not react to light, lack of breathing and pulse - “imaginary death.” Local damage caused by lightning is similar to damage that occurs when exposed to industrial electricity. Dark spots often appear on the skin blue, resembling the branches of a tree (“lightning signs”), which is due to the dilation of blood vessels. When struck by lightning, the general phenomena are more pronounced. Characterized by the development of paralysis, deafness, muteness and respiratory arrest.
 One of the main points when providing first aid is to immediately stop the electric current. This is achieved by turning off the current (turning the switch, switch, plug, breaking wires), removing electrical wires from the victim (with a dry rope, stick), grounding or bridging the wires (connecting two current-carrying wires). Touching a victim with unprotected hands while the electric current dangerous. Having separated the victim from the wires, it is necessary to carefully examine him. Local injuries should be treated and covered with a bandage, as for burns.
One of the main points when providing first aid is to immediately stop the electric current. This is achieved by turning off the current (turning the switch, switch, plug, breaking wires), removing electrical wires from the victim (with a dry rope, stick), grounding or bridging the wires (connecting two current-carrying wires). Touching a victim with unprotected hands while the electric current dangerous. Having separated the victim from the wires, it is necessary to carefully examine him. Local injuries should be treated and covered with a bandage, as for burns.
In case of damage accompanied by light general phenomena (fainting, short-term loss of consciousness, dizziness, headache, pain in the heart), first aid consists of creating peace and transporting the patient to a medical facility. It must be remembered that the general condition of the victim can sharply and suddenly deteriorate in the coming hours after the injury: disturbances in the blood supply to the heart muscle, secondary shock phenomena, etc. occur. Similar conditions sometimes observed even in the affected person with the mildest general symptoms (headache, general weakness); therefore, all persons who have received an electrical injury are subject to hospitalization. As first aid, painkillers (0.25 g amidopyrine, 0.25 g analgin), sedatives (Bechterew's mixture, valerian tincture), cardiac medications (Zelenin drops, etc.) can be given.
In case of severe general phenomena, accompanied by respiratory distress or cessation, the development of a state of “imaginary death”, the only effective first aid measure is immediate artificial respiration, sometimes for several hours in a row. With the heart beating, artificial respiration quickly improves the patient's condition, the skin acquires a natural color, a pulse appears, and blood pressure begins to be determined. The most effective artificial respiration is mouth to mouth (16-20 breaths per minute).
After the victim regains consciousness, he must be given something to drink (water, tea, compote, but not alcoholic drinks and coffee), and covered warmly.
In cases where careless contact with an electrical wire occurred in a hard-to-reach place - on a power transmission tower, on a pole - it is necessary to begin providing assistance with artificial respiration, and in case of cardiac arrest, apply 1-2 blows to the sternum in the area of the heart and take measures to lower it as quickly as possible the victim to the ground, where effective resuscitation can be carried out.
First aid for cardiac arrest should be started as early as possible, i.e. in the first 5 minutes, when the cells of the brain and spinal cord are still living. Help consists of simultaneous artificial respiration and external cardiac massage. It is recommended to continue cardiac massage and artificial respiration until full recovery their functions or the appearance of obvious signs of death. If possible, cardiac massage should be combined with the administration of cardiac drugs.
The victim is transported in a lying position. When transporting to a medical facility victims who are in unconscious or with spontaneous breathing not fully restored, artificial respiration cannot be stopped.
Burying someone struck by lightning into the ground is strictly prohibited.
3.9 Heat (sun)stroke.
Heatstroke- severe pathological condition caused by general overheating body. There are heat strokes caused by predominant exposure to high temperatures. environment, as well as heat stroke resulting from intense physical work(even in comfortable conditions). Along with heat stroke, there is also sunstroke, which is caused by intense or prolonged direct exposure to the body. solar radiation. Clinical picture and pathogenesis heatstroke And sunstroke similar. Predisposing factors are psycho-emotional stress, difficulty in heat dissipation (thick clothing, staying in poorly ventilated rooms), excess weight, smoking, alcohol intoxication, endocrine disorders, cardiovascular diseases, neurological disorders, the use of some medicines etc.
Emergency assistance should be aimed at cooling the body as quickly as possible. For this purpose, both general (immersion in a bath of water at 18-20°, wetting the victim’s skin with water at room temperature and blowing with warm air) and local hypothermia (ice on the head, axillary and groin areas, wiping with sponges moistened with alcohol). When cooling, the victim often experiences motor and mental agitation.
If breathing stops or is suddenly disrupted, it is necessary to start artificial ventilation of the lungs. When the patient comes to his senses, give him a cool, plentiful drink (strongly brewed iced tea).
Treatment of the victim should be carried out in a specialized medical institution, but measures aimed at cooling the body must begin during transportation of the affected person.
4. Transportation of victims.
 The most important task of first aid is to organize fast, safe, gentle transportation (delivery) of a sick or injured person to a medical institution. Causing pain during transportation contributes to the deterioration of the victim’s condition and the development of shock. The choice of transportation method depends on the condition of the victim, the nature of the injury or illness, and the capabilities of the first aid provider.
The most important task of first aid is to organize fast, safe, gentle transportation (delivery) of a sick or injured person to a medical institution. Causing pain during transportation contributes to the deterioration of the victim’s condition and the development of shock. The choice of transportation method depends on the condition of the victim, the nature of the injury or illness, and the capabilities of the first aid provider.
In the absence of any transport, the victim should be transported to a medical facility on a stretcher, including an improvised one. First aid has to be provided even in such conditions when there are no available means or there is no time for  making improvised stretchers. In these cases, the patient must be carried in his arms. First aid also has to be provided in conditions where there are no available means or there is no time to make an improvised stretcher. In these cases, the patient must be carried in his arms. One person can carry the patient in his arms, on his back, on his shoulder.
making improvised stretchers. In these cases, the patient must be carried in his arms. First aid also has to be provided in conditions where there are no available means or there is no time to make an improvised stretcher. In these cases, the patient must be carried in his arms. One person can carry the patient in his arms, on his back, on his shoulder.
If the patient is conscious and can hold himself on his own, then it is easier to carry him in a locked position.
The stretcher strap makes it much easier to carry by hand or on a stretcher.
 In some cases, the patient can cover a short distance on his own with the help of an accompanying person, who throws the victim’s arm over his neck and holds it with one hand, while the other clasps the patient’s waist or chest.
In some cases, the patient can cover a short distance on his own with the help of an accompanying person, who throws the victim’s arm over his neck and holds it with one hand, while the other clasps the patient’s waist or chest.
The victim can lean on the stick with his free hand. If impossible independent movement the victim and the absence of assistants can be transported by dragging on an improvised drag - on a tarpaulin or raincoat.
Thus, in a wide variety of conditions, the first aid provider can organize the transportation of the victim in one way or another. The leading role in choosing means of transportation and the position in which the patient will be transported or transferred is played by the type and location of the injury or the nature of the disease. To prevent complications during transportation, the victim should be transported in a certain position according to the type of injury.
It is very important that the first aid provider, through his behavior, actions, conversations, spares the patient’s psyche as much as possible, strengthens his confidence in successful outcome diseases.
Conclusion.
At the conclusion of the study, the following thesis is irrefutable - regardless of the type of activity and profession of a person, every citizen should be able to provide first aid to the best of his abilities and capabilities. The life and health of an injured person depend on the provision of first aid by persons without special medical education; therefore, it is necessary that every citizen is aware of the essence, principles, rules and sequence of first aid. This is also necessary because there are cases when the victim is forced to provide first aid to himself. The essence of first aid is to stop further exposure to traumatic factors, carry out simple measures and ensure prompt transportation of the victim to a medical facility. Its task is to prevent the dangerous consequences of injury, bleeding, infection and shock.
This thesis was used as the basis for the work, allowing us to reveal the topic of the test in the following sequence:
1. A general historical overview of first aid measures is given.
2. Theoretical aspects of first aid are considered.
3. The practical application of publicly available first aid measures is considered in the context of each type of advent that has a negative impact on human life and health.
4. Methods are given from Ilyin N. Self-help. Directory of emergency first aid. – M. - St. Petersburg, 2000.transportation of the victim, since correctly provided first aid saves the life and health of a person, however, one should not forget about the further rehabilitation of the person in a specialized medical institution, delivery to which falls on the shoulders of the “rescuer”.
List of used literature
1. Life safety. Textbook /Edited by S.V. Belova / M: Higher School, 1999.
2. Ezhov V. First aid. Until the ambulance arrived. – St. Petersburg: Publishing House “Ves”, 2003.
3. Ilyina N. Self-help. Directory of emergency first aid. – M. - St. Petersburg, 2000.
4. First medical aid http://www.firstmedaid.info/raneniya,-travmi.html
5. Instructions for first aid before medical attention emergency care to the victims http://www.ihelpers.narod.ru
We use the expression “throw a tantrum” very often, but few people think about the fact that this is not simple behavioral promiscuity, but a real disease, with its own symptoms, clinic and treatment.
What is a hysterical attack?
A hysterical attack is a type of neurosis manifested by indicative emotional states (tears, screams, laughter, arching, wringing of hands), convulsive hyperkinesis, periodic paralysis, etc. The disease has been known since ancient times; Hippocrates described this disease, calling it “rabies of the uterus,” which has a very clear explanation. Hysterical fits are more typical for women, they are less likely to bother children and occur only as an exception in men.
Professor Jean-Martin Charcot shows students a woman in a hysterical fit
At the moment, the disease is associated with a certain personality type. People subject to attacks of hysteria are suggestible and self-hypnosis, prone to fantasizing, unstable in behavior and mood, love to attract attention with extravagant actions, and strive to be theatrical in public. Such people need spectators who will babysit and care for them, then they receive the necessary psychological release.
Often, hysterical attacks are associated with other psychosomatic deviations: phobias, dislike of colors, numbers, pictures, conviction of a conspiracy against oneself. Hysteria affects approximately 7-9% of the world's population. Among these people there are those who suffer from severe hysteria - hysterical psychopathy. The seizures of such people are not a performance, but a real disease that you need to know, and also be able to provide assistance to such patients. Often the first signs of hysteria appear already in childhood, therefore, parents of children who react violently to everything, bend over backwards, and scream angrily should be shown to a pediatric neurologist.
In cases where the problem has been growing over the years and is pronounced hysterical neuroses an adult is already suffering, only a psychiatrist can help. An examination is carried out individually for each patient, an anamnesis is collected, tests are taken and, as a result, specific treatment is prescribed that is suitable only for this patient. As a rule, these are several groups of drugs (hypnotics, tranquilizers, anxolytics) and psychotherapy.
Psychotherapy in this case is prescribed to open those life circumstances that influenced the development of the disease. With its help, they try to level out their significance in a person’s life.
Symptoms of hysteria

A hysterical attack is characterized by an extreme variety of symptoms
A hysterical attack is characterized by an extreme variety of symptoms. This is explained by the self-hypnosis of patients, “thanks to” which patients can depict the clinic of almost any disease. Seizures occur in most cases after an emotional experience.
Hysteria is characterized by signs of “rationality”, i.e. the patient experiences only the symptom that he “needs” or is “beneficial” at the moment.
Hysterical attacks begin with hysterical paroxysm, which follows an unpleasant experience, a quarrel, or indifference on the part of loved ones. A seizure begins with the corresponding symptoms:
- Crying, laughing, screaming
- Pain in the heart area
- Tachycardia (rapid heartbeat)
- Feeling short of air
- Hysterical ball (feeling of a lump rolling up to the throat)
- The patient falls, convulsions may occur
- Hyperemia of the skin of the face, neck, chest
- Eyes are closed (when trying to open, the patient closes them again)
- Sometimes patients tear their clothes, hair, and hit their heads
It is worth noting features that are not characteristic of a hysterical attack: the patient has no bruises, no bitten tongue, the attack never develops in a sleeping person, there is no involuntary urination, the person answers questions, there is no sleep.
Sensitivity disorders are very common. The patient temporarily ceases to feel parts of the body, sometimes cannot move them, and sometimes experiences severe pain in the body. The affected areas are always varied, it can be the limbs, the abdomen, sometimes there is a feeling of a “driven nail” in a localized area of the head. The intensity of the sensitivity disorder varies, from mild discomfort to severe pain.
Sensory organ disorder:
- Visual and hearing impairment
- Narrowing of visual fields
- Hysterical blindness (can be in one or both eyes)
- Hysterical deafness
Speech disorders:
- Hysterical aphonia (lack of sonority of voice)
- Muteness (cannot make sounds or words)
- Chant (syllable by syllable)
- Stuttering
A characteristic feature of speech disorders is the patient’s willingness to enter into written contact.
Movement disorders:
- Paralysis (paresis)
- Inability to perform movements
- Unilateral paresis of the arm
- Paralysis of the muscles of the tongue, face, neck
- Trembling of the whole body or individual parts
- Nervous tics of facial muscles
- Arching the body
It should be noted that hysterical seizures do not mean real paralysis, but an elementary inability to make voluntary movements. Often, hysterical paralysis, paresis, and hyperkinesis disappear during sleep.
Disorder of internal organs:
- Lack of appetite
- Swallowing disorder
- Psychogenic vomiting
- Nausea, belching, yawning, cough, hiccups
- Pseudoappendicitis, flatulence
- Shortness of breath, imitation of an attack bronchial asthma
At the core mental disorders lies the desire to always be the center of attention, excessive emotionality, inhibition, psychotic stupor, tearfulness, a tendency to exaggerate and the desire to play a leading role among others. All the patient’s behavior is characterized by theatricality, demonstrativeness, and to some extent infantilism; one gets the impression that the person is “glad about his illness.”
Hysterical seizures in children
Symptomatic manifestations of mental seizures in children depend on the nature psychological trauma and on the patient’s personal characteristics (suspiciousness, anxiety, hysteria).
The child is characterized by increased sensitivity, impressionability, suggestibility, selfishness, mood instability, and egocentrism. One of the main features is recognition among parents, peers, society, the so-called “family idol”.
For young children, it is common to hold their breath when crying, provoked by the child’s dissatisfaction or anger when his requests are not satisfied. In older age, the symptoms are more varied, sometimes similar to attacks of epilepsy, bronchial asthma, and suffocation. The seizure is characterized by theatricality and lasts until the child gets what he wants.
Less commonly observed are stuttering, neurotic tics, blinking tics, whining, and tongue-tiedness. All these symptoms arise (or intensify) in the presence of persons towards whom the hysterical reaction is directed.
A more common symptom is enuresis (bedwetting), more often due to changes in the environment ( new kindergarten, school, home, the appearance of a second child in the family). Temporarily removing the baby from a traumatic environment can lead to a decrease in diuresis attacks.
Diagnosis of the disease
The diagnosis can be made by a neurologist or psychiatrist after the necessary examination, during which an increase in tendon reflexes and tremor of the fingers are noted. During the examination, patients often behave unbalanced, may groan, scream, demonstrate increased motor reflexes, spontaneously shudder, and cry.
One of the methods for diagnosing hysterical seizures is color diagnostics. The method represents the rejection of a certain color during the development of a particular condition.
For example, a person dislikes the color orange; this may indicate low self-esteem, problems with socialization and communication. Such people usually do not like to appear in crowded places; it is difficult for them to find a common language with others and make new acquaintances. Rejection of the color blue and its shades indicates excessive anxiety, irritability, and agitation. Dislike for the color red indicates disturbances in the sexual sphere or psychological discomfort that arose against this background. Color diagnostics is currently not very common in medical institutions, but the technique is accurate and in demand.
First aid
It is often difficult to understand whether the person in front of you is sick or an actor. But despite this, it is worth knowing the mandatory first aid recommendations in this situation.

Don’t persuade the person to calm down, don’t feel sorry for him, don’t be like the patient and don’t panic yourself, this will only encourage the hysteroid even more. Be indifferent, in some cases you can go to another room or room. If the symptoms are violent and the patient does not want to calm down, try to splash cold water on his face, bring him to inhale ammonia fumes, give a gentle slap in the face, press on pain point in the cubital fossa. Do not indulge the patient under any circumstances; if possible, remove strangers or take the patient to another room. After this, call your doctor before arriving medical worker don't leave the person alone. After an attack, give the patient a glass of cold water.
During an attack, you should not hold the patient’s arms, head, neck or leave him unattended.
To prevent attacks, you can take courses of tinctures of valerian, motherwort, and use sleeping pills. The patient’s attention should not be focused on his illness and its symptoms.
Hysterical seizures first appear in childhood or adolescence. With age clinical manifestations smooth out, but in the menopause they can again remind themselves and worsen. But with systematic observation and treatment, exacerbations pass, patients begin to feel much better, without seeking help from a doctor for years. The prognosis of the disease is favorable if the disease is detected and treated in childhood or adolescence. We should not forget that hysterical fits may not always be a disease, but only a personality trait. Therefore, it is always worth consulting with a specialist.
Related posts:
No similar entries found.
Guys, we put our soul into the site. Thank you for that
that you are discovering this beauty. Thanks for the inspiration and goosebumps.
Join us on Facebook And VKontakte
Since childhood, we have been taught about how to provide first aid by our parents, school and the Internet. Among such an abundance of advice, it is difficult to understand where the truth is and where the lies are. This information could cost someone’s life, so it’s worth figuring out once and for all how you can help, and what exactly you shouldn’t do.
We are in website We collected several common mistakes when providing first aid and firmly learned what not to do. We hope that there will be no case in our life or in yours when these tips will come in handy, but they are still worth knowing. Just in case.
Myth No. 8. A burn needs to be lubricated with oil.
Many of us were taught this by our grandmothers, but doctors have long disputed this myth. Oil, ointment and even Panthenol create a film and prevent the burn from healing. To quickly cope with this problem, you need to hold the burned area under water for 15-20 minutes and let the wound dry. Only the next day or even later can you apply Panthenol to the burn.
Myth No. 7. The main thing is to apply a tourniquet, but it doesn’t matter how
It seems that the injury was caused by an incorrectly applied tourniquet. more people than from bleeding. The main mistake is applying a tourniquet directly to the skin. This should not be done under any circumstances, as the skin can be seriously damaged. The second mistake is applying a tourniquet to for a long time. At least once an hour, and better time In 20 minutes you need to loosen the tourniquet so that blood flows into the limb. If this is not done, it may even lead to amputation.
Myth No. 6. A pedestrian injured in an accident must be removed from the roadway.
This should not be done under any circumstances, as the victim’s spine may be damaged. The slightest movement with such an injury can lead to disability or even death. In this situation, you need to fence off the scene of the incident with available objects so that passing cars can see the obstacle from afar, and call an ambulance.
Myth No. 5. To apply a splint, you need to straighten the limb and tie it to a stick.
Broken limbs cannot be straightened by force. It is necessary to immobilize the two closest joints by applying a splint so that the victim does not have to straighten his arm or leg.
Myth No. 4. Everyone has this medicine in their medicine cabinet, it definitely won’t make you worse.
An unconscious victim should not be given any medicine, even if it is something familiar to everyone. Each person is individual, and he may be allergic to even the most common drugs. It is better to wait for doctors, trying to help without drug intervention.
Myth No. 3. You need to offer a person a drink: he needs to calm down.
The use of alcohol as an anesthetic is just a common myth. Alcohol thins the blood and increases bleeding. Exactly from medical alcohol, which surgeons gave to patients as a painkiller in the 18th–19th centuries, died huge amount people. In addition, strong alcohol causes intoxication in an already weakened body and interferes with the effect of medical anesthesia.
Myth No. 2. If a person faints, he needs to be brought out of this state urgently
This is a completely wrong judgment. Fainting - defensive reaction body, a kind of reboot. It usually lasts 1–5 minutes. If you hit a person on the cheeks or, for example, pour water on him, you can only worsen the situation and even bring the victim into a coma. In case of fainting









