Position of the humerus. Anatomy: Humerus
The shoulder refers to the long tubular bones of humans. The anatomy is simple and is determined by a number of functions performed. On its surface there are anatomical formations, such as the head, medial condyle, as well as tubercles and pits, which serve as attachment points for muscles and ligaments. The humerus functions as a lever. Fractures are very dangerous, because due to damage to the bone marrow canal, a fat embolism can develop or a vessel may become blocked.
Most often, the shoulder suffers as a result of fractures in the area of the anatomical neck.
Structure and anatomy
At the top of the bone there is a round formation - the head, which is an integral part of the joint. It is separated from the rest of the bone by a narrow groove. It is called the anatomical neck. It is in this part that fractures most often occur. Behind it is the place of attachment of the main muscles of the shoulder, represented by two tubercles - large and small, as well as ridges. The lesser tubercle is located in front of the shoulder. There is a tuberosity in the middle of the bone. This is where the deltoid muscle attaches. On the side of the elbow, the humerus ends with 2 epicondyles, between which there is an articular surface. The medial condyle is much larger than the lateral one. There are also 2 recesses located here - the olecranon process or ulnar fossa and the radial one.
Functions of the humerus
The shoulder structure is actually a lever and increases the range of motion of the upper limb. In addition, the bone is involved in maintaining balance when the center of gravity shifts while walking. This element determines the correct support of a person on his hands when climbing stairs and in other specific body positions.
Damage: causes and symptoms
 When the shoulder joint is dislocated, a person feels sharp pain.
When the shoulder joint is dislocated, a person feels sharp pain. Dislocation of the shoulder and elbow joint is common and is associated with high mobility of the upper limb. There are anterior, posterior and inferior displacement. If damaged, it becomes difficult to move the limb, pain is felt, and swelling is visualized. When a nerve is pinched, the skin becomes numb. Dislocations are distinguished as new and old. At the same time, a protrusion of the greater tubercle or a fracture of the neck may occur. The shoulder is swollen, painful, there is noticeable hemorrhage, sensitivity in the arm and fingers is lost.
A fracture of the humerus occurs due to significant force. This happens when you fall backward on your elbows or forward on your outstretched arms. Bone fracture occurs in anatomically weak areas. These include:
- anatomical and surgical neck;
- condyle area;
- area of the head of the humerus;
- the middle of the bone.
Immediately after the injury, the patient feels a sharp pain in the arm, as well as the inability to perform actions with it. The exact amount of movement lost depends on the immediate location of the injury. After some time, severe swelling of the shoulder is observed, and bruising and bruising may develop. In this case, the limb is significantly deformed.
Diseases
 Among the diseases of this joint, arthritis is common.
Among the diseases of this joint, arthritis is common. A common disease is the introduction of infection into the bone marrow through the blood. Damage to the shoulder occurs because this bone is tubular and has an abundant blood supply. As a result of the development of this disease, bone tissue can decompose, and then pathological fractures form (without the participation of strong external influences). In addition, it is possible to develop arthritis of the shoulder and elbow joint.
To perform the functions of support, movement and protection, our body has a system that includes bones, muscles, tendons and ligaments. All its parts grow and develop in close interaction. Their structure and properties are studied by the science of anatomy. The humerus is part of the free upper limb and, along with the bones of the forearm and the scapula and clavicle, provides complex mechanical movements of the human arm. In this work, using the example of the humerus, we will study in detail the principles of the musculoskeletal system and find out how its structure is related to the functions it performs.
Features of tubular bones
A triangular or cylindrical shape is characteristic of the components of the skeleton - tubular bones, in which elements such as the epiphyses (edges of the bone) and its body (diaphysis) are distinguished. Three layers - the periosteum, the bone itself and the endosteum - are part of the diaphysis of the humerus. The anatomy of the free upper limb is currently quite well studied. It is known that the epiphyses contain spongy substance, while the central section is represented by bone plates. They form a compact substance. The long shoulder, elbow, and femur have this appearance. The anatomy of the humerus, a photo of which is presented below, indicates that its shape best corresponds to the formation of movable joints with the bones of the upper limb girdle and forearm.

How do tubular bones develop?
During the process of embryonic development, the humerus, together with the entire skeleton, is formed from the middle germ layer - the mesoderm. At the beginning of the fifth week of pregnancy, the fetus has mesenchymal areas called anlages. They grow in length and take the form of humeral tubular bones, the ossification of which continues after the birth of the child. The top of the humerus is covered with periosteum. This is a thin shell consisting of connective tissue and having an extensive network of blood vessels and nerve endings that enter the bone itself and provide its nutrition and innervation. It is located along the entire length of the tubular bone and forms the first layer of the diaphysis. As anatomy science has established, the humerus, covered with periosteum, contains fibers of the elastic protein - collagen, as well as special cells called osteoblasts and osteoclasts. They are grouped near the central channel of Havers. With age, it fills with yellow bone marrow.

Self-healing, repair and growth in thickness of tubular bones in the human skeleton is carried out thanks to the periosteum. The anatomy of the humerus in the middle part of the diaphysis is specific. There is a tuberous surface to which the superficial deltoid muscle is attached. Together with the girdle of the upper limbs and the bones of the shoulder and forearm, it ensures the lifting and abduction of the elbows and arms up, back and in front.
The significance of the epiphyses of tubular bones
The end parts of the tubular bone of the shoulder are called epiphyses, contain red bone marrow and consist of spongy substance. Its cells produce blood cells - platelets and red blood cells. The epiphyses are covered with periosteum and have bone plates and cords called trabeculae. They are located at an angle to each other and form an internal skeleton in the form of a system of cavities, which are filled with hematopoietic tissue. How to determine the bones at the junction with the scapula and the bones of the forearm is quite complex. The articular surfaces of the humerus have proximal and distal ends. The head of the bone has a convex surface that is covered and fits into the socket of the scapula. A special cartilaginous formation of the scapular cavity - the articular lip - serves as a shock absorber, softening shocks and impacts when the shoulder moves. The capsule of the shoulder joint is attached at one end to the scapula, and at the other to the head of the humerus, descending to its neck. It stabilizes the connection between the shoulder girdle and the free upper limb.
Features of the shoulder and elbow joints
As human anatomy has established, the humerus is part of not only the spherical shoulder joint, but also another one - the complex elbow joint. It should be noted that the shoulder joint is the most mobile in the human body. This is understandable, since the hand serves as the main instrument of labor operations, and its mobility is associated with adaptation to upright posture and freedom from participation in movement.

The elbow joint consists of three separate joints connected by a common joint capsule. The distal humerus articulates with the ulna to form the trochlear joint. At the same time, the head of the condyle of the humerus enters the fossa of the proximal end of the radius, forming the humeroradial mobile joint.
Additional shoulder structures
The normal anatomy of the humerus includes the greater and lesser apophyses, the tubercles from which the ridges arise. They serve as an attachment point. There is also a groove that serves as a container for the biceps tendon. At the border with the body of the bone, the diaphysis, below the apophyses, the surgical neck is located. It is most vulnerable to traumatic shoulder injuries - dislocations and fractures. In the middle of the body of the bone there is a tuberous area to which the deltoid muscle is attached, and behind it there is a spiral-shaped groove in which the radial nerve is immersed. At the border of the epiphyses and diaphysis there is a region whose rapidly dividing cells determine the growth of the humerus in length.
Humerus dysfunction
The most common injury is a fracture of the shoulder due to a fall or severe mechanical shock. The reason is that the joint does not have real ligaments and is stabilized only by the muscular corset of the upper limb belt and an auxiliary ligament, which looks like a bundle of collagen fibrils. Soft tissue lesions such as tendinitis and capsulitis are quite common. In the first case, the tendons of the supraspinatus, infraspinatus, and teres minor muscles are damaged. Another disease occurs as a result of inflammatory processes in the joint capsule of the shoulder.

The pathologies are accompanied by tunnel pain in the arm and shoulder, limited mobility of the shoulder joint when raising the arms up, placing them behind the back, or abducting them to the sides. All these symptoms sharply reduce a person’s performance and physical activity.
In this article, we studied the anatomical structure of the humerus and found out its relationship with the functions performed.
The scapula and humerus take part in the formation of the shoulder joint. Therefore, first of all, it is advisable to consider the anatomical formations of these bones associated with the topography of the shoulder joint. The outer angle of the scapula is represented by the glenoid cavity(cavitas glenoidalis), above and below which the supraglenoid is located(tuberculum supraglenoidale) and subarticular (tuberculum infraglenoidale) tubercles. The coracoid process is located on the upper edge near the outer corner(processus coracoideus), medial to which there is a notch of the scapula(incisura scapulae). The coracoid process and subarticular tubercle are separated from the glenoid cavity by the neck of the scapula(collum scapulae). Spine of the scapula (spina scapulae), goes into acromion(acromion) having an angle (angulus acromialis).


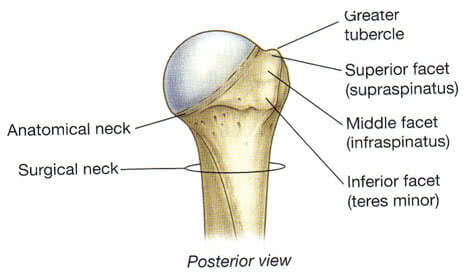
IN proximal end of the humerus (oshumerus) distinguish the head, the anatomical neck, the greater and lesser tubercles, the intertubercular groove, and the surgical neck. Head of humerus (caputhumeri) covered with hyaline cartilage. Anatomical neck (withllitanatomicum) separates the head of the humerus from the rest of it. Greater tuberosity { tuberculummajus) located on the lateral surface of the humerus and serves as the attachment point for the supraspinatus (T.supraspinatus), infraspinatus (T.infraspinatus) and teres minor muscles (T.teresmajor), providing external rotation of the shoulder. Lesser tubercle (tuberculumminus) located on the anterior surface of the humerus and serves as the attachment point for the subscapularis muscle (T.subscapularis). Intertubercular groove (sulcusintertubercularis) located between the greater tuberosity and the crest of the greater tuberosity (cristatuberculimajoris) on one side and the lesser tubercle and the crest of the lesser tuberosity (cristatuberculiminoris) on the other, in which the tendon of the long head of the biceps brachii passes (T.bicepsbrachii). Surgical neck (collumchirurgicum) located below the tubercles and corresponds to the location of the epiphyseal cartilage.
Shoulder joint (ariiculatiohumeri) formed by the head of the humerus (caputhumeri) and the glenoid cavity of the scapula (cavitas glenoidalis scapulae).
The size of the glenoid cavity is four times smaller than the head of the humerus, and its volume is increased by the cartilaginous articular lip (labrum glenoidale), which is also a shock absorber that softens sudden movements in the joint. However, remaining incongruity is the cause of humeral dislocations.
Between the outer end of the coracoid process and the middle part of the inner surface of the acromion there is a dense, 0.8-1 cm wide lig. coracoacromiale. Located above the joint, this ligament, together with the acromion and coracoid process, forms the arch of the shoulder. The arch limits the upward abduction of the shoulder in the shoulder joint to a horizontal level. The hand rises higher along with the shoulder blade.
Shoulder joint space projected in front onto the apex of the coracoid process (palpated below the outer part of the clavicle in the depths of the sulcus deltopectoralis), externally - along the line connecting the acromial end of the clavicle with the coracoid process, behind - under the acromion, in the interval between the acromial and spinous parts of the deltoid muscle
Projection of the joint space of the shoulder joint from the outside and from the back
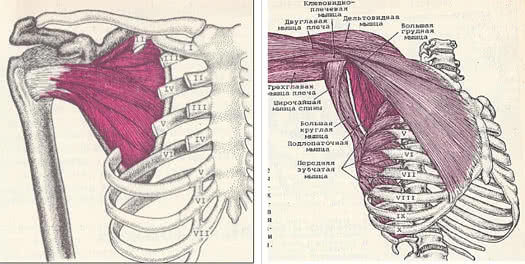
Muscles. The main role in strengthening the shoulder joint and its capsule belongs to the muscles.
From below from the joint, without covering the capsule, there is a long head m. triceps, starting from tuberculum infraglenoidae.
From outside and from above the joint is covered by the deltoid muscle, which is not directly connected to the joint capsule. The muscle consists of a posterior (spinous) part, starting from the scapular spine, a middle (acromial) part, starting from the acromion, and an anterior (clavicular) part. After the fibers of the muscle converge, a common tendon attaches to the deltoid tuberosity of the humerus.
The long head tendon is located under the deltoid muscle. biceps brachii, starting on the tuberculum supraglenoidale and passing through the joint cavity. The tendon limits the upward and anterior movements of the humeral head and holds the articular ends of the bones.
The tendon then lies in the intertubercular groove, surrounded by the intertubercular synovial sheath and then connects to short head, starting from the coracoid process.
Joint front covers 1) short headm.biceps 2) passing next to her m.coracobrachialis(starts from the apex of the coracoid process, and attaches below the middle of the medial surface of the humerus along the crest of the lesser tubercle. F-raises the arm and leads to the midline), 3) m.subscapularis starting in the subscapular fossa, attaching to the lesser tubercle and its crest. The tendon fuses with the anterior surface of the capsule of the shoulder joint, which the muscle retracts during contraction. In cases where the tendon of the subscapularis muscle with its upper part passes into the joint cavity, the upper anterior wall of the latter turns out to be somewhat weakened. F – pronates the shoulder and participates in bringing it to the body. Innervation n. subscapularis (C5-C7). Blood supply a. Subscapularis. and also 4) the most superficially located m.pectoralismajor which starts from the clavicle, sternum, cartilages of ribs 2-7, attaching to the crest of the greater tubercle. F- adducts and internally rotates the shoulder. Innervation n. pectoralis medialis et lateralis (C5-Th 1). Blood supply a. thoracoacromialis, thoracica lateralis.
Behind and on top of the shoulder joint is covered by a tendon m.supraspinatus, which begins in the supraspinatus fossa, passes under the acromion, attaching to the greater tubercle of the humerus. The terminal tendon fuses with the posterior surface of the articular capsule and, when contracted, pulls it back, preventing pinching. F- abducts the shoulder, turning it slightly outward. Innervation n. Suprascapularis (C5-C6). Blood supply a. Suprascapularis, circumflexa scapula.
Behind The shoulder joint also contains a tendon m.infraspinatus, which starts from almost the entire surface of the infraspinatus fossa and is attached to the greater tubercle of the humerus below the place of attachment of m. supraspinatus and above the tendon attachment m. teres minor. The infraspinatus muscle is fused with the capsule, covered on top by the deltoid and trapezius muscles, and in the lower sections by the latissimus dorsi and teres major muscles. F- takes the raised arm back and rotates the shoulder outward. Innervation n. Suprascapularis (C5-C6). Blood supply a. Suprascapularis, circumflexa scapula.
Besides, behind the shoulder joint is covered by a tendon m.teresminor starting from the lateral edge of the scapula and attaching to the greater tubercle of the humerus. The tendon fuses with the posterior surface of the articular capsule of the shoulder joint and, when contracted, retracts the capsule. F- supinates the shoulder (rotates the shoulder outward) slightly moving it posteriorly. Innervation of n.axillaris (C5-C6). Blood supply a. circumflexa scapula.
Thus, from above and behind the joint capsule is strengthened by ligaments and tendons of muscles, but from below and from the inside there is no such strengthening. This is largely responsible for the fact that in most cases the head of the humerus dislocates forward and inward.
Articular capsule of the shoulder joint loose and relatively thin. It is attached on the scapula to the bony edge of the glenoid cavity and, covering the head of the humerus, ends at the anatomical neck. In this case, both tubercles remain outside the joint cavity.
Articular capsule of the shoulder joint. Rear view And.
From the inside and below, the articular capsule is attached much lower, at the level of the surgical neck of the shoulder, forming the so-called axillary inversion, recessus axillaris.
Fibrous layer of the joint capsule has thickened and weak areas. Thickened ones are formed due to bundles, the most pronounced of them is lig. coracohumerale, starting from the outer edge of the coracoid process and heading to the greater and, to a lesser extent, to the lesser tuberosity of the humerus. Moreover, most of its fibers are woven into the capsule in the upper and back parts. The ligament is located between the tendons of the supraspinatus and subscapularis muscles. Non-permanent occurs in 59% of cases.
Ligaments and arch of the shoulder
The so-called glenohumeral ligaments, ligg. glenohumerale, or Flood's ligaments[Flood], top, middle and bottom. They are stretched between the anatomical neck and labrum glenoidale. Between the ligaments"weak points" remain. The capsule between the middle and inferior ligaments is especially thin - this place is the anterior “weak spot” of the capsule. In the absence of the middle ligament (occurs in 1/6 cases), a dislocation in the shoulder joint can easily occur.
Flood's ligaments and intertubercular volvulus

Inversions. The cavity of the shoulder joint is expanded due to three twists(protrusions of the synovial membrane): axillary, intertubercular and subscapular. During torsions, the joint capsule is least resistant to pressure from the fluid accumulated in its cavity, and with purulent omartritis, this is where pus breaks through into neighboring areas, forming periarticular leaks.
Axillary volvulus(recessus axillaris) corresponds to the anterior inferior section of the capsule, which is located in the gap between the subscapularis and the beginning of the long head of the triceps muscle and descends to the surgical gap of the shoulder. Immediately inward from the axillary volvulus, at the point of its attachment to the surgical neck, the axillary nerve passes, which, when dislocated, is often damaged and involved in the process of arthritis. At the back, the axillary inversion is covered by the m.teres minor, which allows one to approach it through the gap between this muscle and the infraspinatus without coming into contact with the axillary nerve passing through the quadrilateral foramen. The axillary volvulus, being looser and lower located, can serve as the main place for the accumulation of pus during inflammation of the joint. Paths of spread of purulent leaks from the axillary inversion down through the 3rd or 4th side opening into the axillary fossa or along the long head of the triceps into the posterior fascial bed of the shoulder.
Intertubercular volvulus represents essentially the synovial sheath of the tendon of the long head of the biceps. It lies on the anterolateral surface of the proximal end of the humerus in the intertubercular groove. In this area, the articular capsule is thrown over the groove in the form of a bridge, and then only its synovial layer continues into the groove, forming a finger-like pocket surrounding the tendon of the long head of the biceps brachii muscle, ending blindly at the level of the surgical neck of the humerus. Due to the tight covering of the intertubercular volvulus by tendons, pus rarely breaks through it. If this happens, then pus enters the subdeltoid space and the anterior fascial bed of the shoulder with secondary leaks along the neurovascular bundles.
Subscapular inversion is located at the level of the anterior superior section of the neck of the scapula and is a synovial bursa of the subscapularis muscle, ( bursasynovialissubscapularis) located on the anterior surface of the joint capsule under the upper section of the tendon of the subscapularis muscle and always communicating with the joint cavity by one or two holes. When the subscapularis volvulus ruptures, pus spreads posteriorly and medially into the subscapularis osteofibrous bed or into the axilla.
Bags and wraps

Synovial bursae. Around the joint there is a significant number of synovial bursae, which make up the sliding apparatus of the muscle-tendon formations.
In addition to the already known bursasynovialissubscapularis(subscapularis inversion) located on the border of the deltoid and subclavian regions, between the neck of the scapula and the tendon of the subscapularis muscle there is also a higher and more superficial one bursasubcoracoidea, located between the base of the coracoid process and the upper edge of the tendon of the subscapularis muscle. Often the subcoracoid bursa is also the same as the subscapularis reported with the cavity of the shoulder joint.
Location of the synovial bursae in the shoulder joint area. Front view

Often these two bags merge. Bursam.coracobrachialis located under the coracoid process and the beginning of m.coracobrachialis. It often communicates with the joint cavity.
On top of the greater tubercle and the supraspinatus tendon lies a considerable size bursasubdeltoidea, which often communicates with the underlying subacromial bursa (bursa subacromialis). The last bursa is located between the acromion and lig. Coracoacromiale. Both of these bags do not usually communicate with the joint cavity.
bursa subacromialis, bursa subdeltoidea and bursa subtendinea infraspinati
At the site of attachment of the infraspinatus muscle to the greater tubercle there is bursasubtendineainfraspinati(sometimes communicating with the joint cavity).
Transverse section at the level of the humeral head

In the area of the shoulder joint, in addition to those discussed above, there are also a number of synovial bursae that are not associated with the joint cavity. Bursa m. One or two latissimi dorsi subtendinea are located in the area where the muscle attaches to the humerus on its anterior surface. At the site of attachment of the teres major muscle to the crest of the lesser tubercle of the humerus there is a bursa subtendinea m. teretis majoris. Between the crest of the greater tubercle and the tendon of the pectoralis major muscle is the bursa subtendinea m. pectoralis majoris. There is a non-permanent bursa m. supraspinati.
Synovial bursae of the shoulder joint
Synovial bursae play a large role in the pathology of the shoulder joint and can initiate the development of an inflammatory process, both in the joint and in the surrounding cellular spaces.
The constant sources of innervation of the capsule of the shoulder joint are the axillary (C5-C6) and suprascapular nerves (C5-C6).
Damage to the suprascapular nerve is possible due to trauma with significant displacement of the scapula laterally or dorsally.
At the same time, the tunnel syndrome of the suprascapular nerve is known, first described in 1960 by N. Kopell, W. Thompson under the name “trap” neuropathy of this nerve. In order to understand the genesis of the syndrome, it is necessary to consider some topographic and anatomical facts. The suprascapular nerve originates from the superior trunk of the brachial plexus, forming from the C5 and C6 roots. The nerve runs down behind the brachial plexus to the superior edge of the scapula. At the superior edge of the scapula, the nerve passes through the suprascapular notch, transformed into an opening by the superior transverse scapular ligament. After passing through the notch, the nerve reaches the posterior surface of the scapula in the supraspinatus fossa. Here it innervates the supraspinatus muscle and gives articular branches to the shoulder and acromioclavicular joints. Then it wraps around the lateral edge of the spine of the scapula and reaches its end in the infraspinatus muscle, which it also innervates.
The passage of the nerve through the suprascapular foramen is fraught with compression when the nerve is pulled and bent over the edge of the foramen. A similar condition can occur with a forced adduction movement of the arm crossing the midline of the body. This movement causes rotation and displacement of the scapula around the back of the rib cage. This movement increases the tension on the nerve (the distance from the cervical origin of the nerve to the suprascapular notch increases), as a result of which the nerve is subjected to compression. To diagnose suprascapular nerve tunnel syndrome, the “Napoleon pose” (crossing your arms over your chest) is used. In this case, the tensely straightened arm passively moves to the other half of the body, crossing its midline. With this movement, the displacement of the scapula causes extreme pain as a result of tension and pinching of the nerve.
The suprascapular nerve has no cutaneous sensory branches, but carries propriosensitivity from the muscles and joints it innervates. Therefore, when a nerve is compressed, the pain is characterized as deep, “boring,” aching, localized in the area of the scapula along the back and outer surface of the shoulder.
In the diagnosis of suprascapular nerve tunnel syndrome, the appearance of pain on palpation of the projection site of the suprascapular nerve at the entrance to the notch of the scapula is also used.
Damage to the axillary nerve can occur with a dislocated shoulder, with strong traction on the arm to correct the dislocation, ( one out of 7 shoulder dislocations is complicated by nerve palsy due to primary stretching of the branches of the brachial plexus) much less often as an isolated injury. It is manifested by paresis or paralysis of the deltoid muscle, lack of active abduction of the shoulder, loss of skin sensitivity in the deltoid region and along the anterior outer surface of the shoulder. Clinically and radiologically, a downward displacement of the humeral head is determined, which stimulates subluxation or dislocation of the shoulder.
The location of the axillary nerve next to the axillary volvulus does not exclude the transfer of inflammation to the nerve during omartritis.
The passage of the axillary nerve in the quadrilateral foramen causes the possibility of compression of this nerve, because this hole narrows significantly with simultaneous abduction and flexion of the shoulder. Cases of compression of the axillary nerve have been described in dentists who are forced to frequently carry out professional movements (abduction and simultaneous flexion of the shoulder), which led to repeated traumatization of the nerve (Zhulev N.M. et al., 1992)
Blood supply aa. circumflexae humeri anterior et posterior and additionally through the deltoid and acromial branches from a. thoracoacromialis.
Sometimes the displaced head of the humerus presses on the vessels in the armpit. The arm may remain blue and cold until the dislocation is reduced. In rare cases, rupture of the axillary artery and the formation of a traumatic aneurysm occur, especially when attempting to reduce an old dislocation by forceful manipulation.
SOME ASPECTS OF TOPOGRAPHIC ANATOMY OF THE MUSCLES IN THE SHOULDER JOINT AREA
In the area of the shoulder joint there are various anatomical formations (bones, cartilage, muscles, bursae, vessels, nerves, etc.) pathological changes in which can manifest themselves with a variety of clinical symptoms, and it is necessary to begin to understand its nature with a clear understanding of the structure, relative position and functions of these anatomical structures.
The purpose of this short review is to consider some topographic and anatomical features of the structure of the muscle layer of the shoulder joint area.
Pathology of the muscles located in the area of the shoulder joint causes limited mobility and the appearance of pain in areas adjacent to the joint. The cause of muscle pathology is, first of all, acute or chronic injury, which can lead to tendon rupture, or to the development of degenerative changes in muscle, tendon tissue, or even in the joint capsule. The appearance of an isolated focus of tension and pain in the muscle is accompanied by irradiation of pain to nearby anatomical areas. Such conditions are described under different names (muscular rheumatism, myofascial syndrome, myofasciitis etc.). Lesions of individual muscles located next to the shoulder joint have received various names (frozen shoulder, silver dollar pain area symptom, shoulder pain symptom, subdeltoid bursitis mimic etc.).
The shoulder joint has a much wider range of motion than any other joint. The extensible capsule and small flat articular surface allow for such mobility.
Movement in the shoulder joint is carried out around three main axes: around the frontal axes - flexion (movement of the upper limb forward and upward) and extension (movement of the limb backward and upward); around the sagittal - abduction (movement of the limb to the side and upward) and adduction (movement of the limb down to the body); around a vertical axis - rotation of the lowered limb with the palm inward (pronation) and rotation of it with the palm outward (supination). Circular movement (circumduction) is also possible in the joint - movement alternately around many axes, when the entire limb describes the shape of a cone. According to V.A. Gamburtsev (1973), the amplitude (span) of movements in the shoulder joint normally at the age of 10 to 40 years fluctuates within the following limits (initial position - the limb is lowered along the body): flexion - 181-179°; extension – 89-85°; – 184-179°; pronation – 103-102°; supination – 45-42°. Moreover, flexion and abduction above the horizontal position of the limb occur in combination with movements of the shoulder girdle.
The muscles (supraspinatus, infraspinatus, teres minor and subscapularis) that rotate the shoulder formROTATOR CUFF (BasmajianJ.V . 1978).All these muscles, starting on the scapula, are attached to the greater and lesser tubercles of the humerus.
The tendons of the supraspinatus, infraspinatus and subscapularis muscles on each side form a thick continuous layer, fused to the underlying joint capsule and separated from the deltoid muscle and acromion process by a mucous bursa.
An important function of the rotator cuff muscles is stabilization.the head of the humerus in the glenoid fossa during arm movements. With pathology of the muscles that make up the rotator cuff, decentralization of the head can occur, resulting in pain and impaired movement in the shoulder joint.
In this regard, we will consider some of the practical topographic and anatomical features of the structure of each of the muscles that make up the rotator cuff.

SUPRASPINAL MUSCLE the medial end is attached to the supraspinous fossa of the scapula, and the lateral end, passing under the acromion, is attached to the upper part of the greater tubercle of the humerus.

Knowledge of the points of attachment and course of the supraspinatus muscle helps to understand its function, an understanding of which allows us to better understand some aspects associated with the pathology of this muscle. The supraspinatus muscle abducts the shoulder and pulls the head of the humerus medially into the glenoid cavity, which prevents the head from moving downward when the arm is freely lowered. Based on this, the mechanism becomes clear The “falling arm” symptom, pathognomonic for a complete rupture of the supraspinatus tendon. The hand, passively raised to a vertical position, falls when trying to lower it, i.e. the patient cannot actively hold it in the abduction position. With a complete rupture of the supraspinatus tendon, the deltoid muscle alone cannot fully abduct the shoulder and in such patients it becomesactive abduction of the arm is possible only up to 60° due to the movement of the scapula.
The fact that the main function of the supraspinatus muscle is shoulder abduction makes clear the genesis of the main complaint of patients with pathology of this muscle: pain that increases withmovement of the limb to the side and up. And at rest, which is typical, the pain is not intense and is dull in nature.
Impaired shoulder abduction explains the difficulties patients experience when the supraspinatus muscle is damaged when raising their arms to their head to comb their hair, brush their teeth, etc.
When the supraspinatus muscle is damaged, tension in its fibers appears, which disrupts the normal sliding of the head of the humerus in the glenoid fossa. Apparently this explains the crunching or clicking sound in the shoulder joint that occurs in some patients with pathology of the supraspinatus muscle, which disappears after the muscle tension is eliminated.
Features of the topographic-anatomical location of the muscle cause the appearance of pain with pathology of the supraspinatus muscle in the shoulder girdle. Pain is especially pronounced in the middle of the deltoid region. And this localization of pain, given its location above the supraspinatus tendon and greater tubercle of the humerus bursasubdeltoidea ( the size of the bursa corresponds approximately to the patient's palm) is often mistakenly perceived as a symptom of subdeltoid bursitis (subdeltoid bursitis simulator) In these cases, as one of the methods of differential diagnosis, identifying point tenderness in the area of the supraspinatus muscle can help. After finding such points of palpation tenderness, local anesthetics are injected into them for diagnostic and therapeutic purposes. Considering that the supraspinatus muscle is innervated by the suprascapular nerve, it is proposed ( SkillernP. G .), to relieve unexplained pain in the shoulder girdle, accompanied by pain on palpation of the supraspinatus muscle, block the suprascapular nerve.
Location of bursasubdeltoidea, bursasubacromialis relative to m. supraspinatus and acromion
Above the subdeltoid bursa is located between the acromion and lig. coracoacromiale subacromial bursa. Most often these bags communicate with each other. With each abduction of the shoulder in the range from 60 to 120°, friction is created between the supraspinatus tendon and the acromion process, which is reduced due to the presence of the mucous bursa lying between them.
Contact m. supraspinatussacromion during arm abduction


Over time, especially in people engaged in heavy physical labor associated with intense movements of the shoulder, the walls of the bag are damaged, and it ceases to provide sufficient protection. Constant repeated traumatization causes degenerative changes in the tendons and joint capsule. Such degenerative changes predispose to calcification of the supraspinatus tendon. Such deposits increase compression by the acromion process, causing the pain to be much more severe than with simple inflammation of the tendon sheaths. Abraded necrotic fibers are extremely sensitive to any damage and a simple fall or sudden muscle strain can cause incomplete or even complete rupture of the tendons. Degenerative changes can spread to the adjacent long head of the biceps muscle, which spontaneously ruptures, or to the entire capsule tissue, causing periarthritis and the formation of periarticular adhesions. One of the symptoms of inflammation of the supraspinatus tendon may be pain when the shoulder is abducted in the range from 60 to 120°, that is, to the extent that the tendon is pinched by the edge of the acromion process. Beyond this, when the limb is in full abduction, movements cease to be painful, since the sensitive area is protected by the acromion process without coming into contact with it. Likewise, when the shoulder drops down, sharp pain again occurs between 120 and 60° abduction. This symptom may be differentially significant, since with arthritis of the shoulder joint, pain appears immediately with the onset of movement and continues throughout the entire range of movement. With fusions in the shoulder joint, pain occurs when the shoulder is abducted by 70-80°, but continues with further abduction.
SUBSINNATIUS MUSCLE Information about the pathology of the infraspinatus muscle is of particular importance for differential diagnosis in rheumatology. Many authors indicate that pain emanating from the infraspinatus muscle very closely mimics the pain that occurs in the shoulder joint itself (symptom of pain in the shoulder joint), and can be mistaken for symptoms of arthritis of the shoulder joint. When the infraspinatus muscle is affected, the main localization of pain is the anterior region of the shoulder joint, but pain can also be projected down to the anterolateral region of the shoulder. This type of pain requires clarification of the location of the muscle.
The infraspinatus muscle starts from more than 2/3 of the surface of the infraspinatus fossa of the scapula, goes laterally and is attached to the posterior surface of the greater tubercle of the humerus.

Muscle covered on top by the deltoid and trapezius muscles, and in the lower sections by the latissimus dorsi and teres major muscles. Blood supply a. Suprascapularis, circumflexascapula . For pain in the shoulder joint caused by pathology of the infraspinatus muscle, you can use deep palpation to determine areas of local pain in the muscle itself. Most often, pain is detected at a point lying below the lateral border of the medial 1/3 of the scapular spine and equidistant from the spine and medial angle of the scapula, or in an area located below the middle of the scapular spine. In addition, tight cords are sometimes palpated in the area of the affected subscapularis muscle.
Innervation of the muscle is carried out n. suprascapularis , extending through the upper trunk from the 5th and 6th cervical nerves. Pathology of the infraspinatus muscle causes pain in the areas innervated by the 5th, 6th and 7th cervical nerves, which can lead to an erroneous diagnosis of radiculopathy caused by intervertebral disc disease ( ReynoldsM. D. 1981)
The infraspinatus muscle rotates the shoulder outward in any position and is involved in stabilizing the head of the humerus in the glenoid cavity when raising the arm up. In addition, the upper fibers of the muscle are involved in abduction (raised hand is pulled back), and the lower ones in shoulder adduction. The infraspinatus muscle, together with the teres minor muscle and the posterior fibers of the deltoid muscle, rotates the shoulder outward. The infraspinatus muscle helps the supraspinatus and other rotator cuffs stabilize the humeral head in the socket during shoulder abduction and extension.
From our point of view, it is interesting that in the case of myofascial pain reflected in the shoulder joint, the source of this pain, according to some authors, is most often localized in the infraspinatus or supraspinatus muscles. This may be due to the common innervation of these muscles by the suprascapular nerve. It is unlikely that such localization of pain is a direct consequence of the contractile activity of these muscles. After all, the infraspinatus and supraspinatus muscles have different functions, but at the same time they cause deep pain in the shoulder joint; at the same time, the infraspinatus and teres minor muscles perform almost the same actions, but have different innervation and different localization of pain.
Information about the function of the muscle makes it possible to explain the reason for patients’ complaints that they cannot reach the back pocket of their trousers with their hand, cannot fasten their bra, etc. Performing these movements requires internal rotation of the shoulder, which should be accompanied by stretching of the muscles that rotate the shoulder outward. And when the infraspinatus muscle is damaged, leading to tension and shortening of the muscle fibers, the patient is unable to even reach the back pocket of his trousers with his fingers. Moreover, the limitation of this movement is the same for both active and passive execution.
TERESUS MINOR MUSCLE originates from the posterior surface of the lateral edge of the scapula and inserts on the inferior facet of the greater tubercle of the humerus below the infraspinatus tendon. The tendon fuses with the posterior surface of the articular capsule of the shoulder joint and, when contracted, retracts the capsule. Blood supply a. circumflexascapula. Innervation n. axillaris (C 5-C 6).
An isolated lesion of the teres minor muscle is described in the literature as pain area symptom the size of a silver dollar . It is caused by patients complaining of pain in an area the size of a silver dollar (the diameter of an American silver dollar is 32 mm) deep in the posterior portion of the deltoid muscle just proximal to its insertion on the deltoid tuberosity of the humerus. Perhaps the localization of pain in the deltoid region is somehow related to the fact that the teres minor and deltoid muscles are innervated by the same nerve. The pain is perceived by the patient as deep and well-defined and this may be falsely interpreted as bursitis. To make a correct diagnosis, one should take into account the pathognomonic localization of pain in the area located significantly below the subacromial bursa.
The teres minor muscle supinates the shoulder (rotates the shoulder outward), moving it slightly posteriorly. Many authors identify the actions of the teres minor and infraspinatus muscles. Both muscles rotate the shoulder outward, regardless of the position of the arm (abducted, flexed, straightened) and are involved in stabilizing the head of the humerus in the glenoid cavity during arm movements.
Course and topography and m . teresminor


Myofascial syndrome of the teres minor muscle is uncommon ( SolaA . E ). Even more rare is an isolated lesion of the teres minor muscle. As a rule, there is a combined pathology of the teres minor and infraspinatus muscles. Moreover, the pain from the latter is clearly dominant, and the elimination of tension in the infraspinatus muscle helps to detect pain irradiation from the teres minor muscle. Probably, this combination of pathology can be explained by the fact that the teres minor muscle, in the figurative expression of D.G. Trevella, functions as a younger brother in parallel with the infraspinatus muscle. These muscles have adjacent areas of anatomical origin and attachment, but different innervation. The same role of the “little brother” can probably explain the fact that with an isolated lesion of the teres minor muscle, patients complain more of pain than of limited movement. Probably, compensation of movements occurs due to the infraspinatus muscle.
SUBSCLATURE MUSCLE starts from the anterior surface of the scapula, filling the subscapular fossa from the medial to the lateral edge. Directing laterally, it passes into a tendon that crosses the front of the shoulder joint and attaches to the lesser tubercle of the humerus and to the infero-anterior part of the articular capsule of the shoulder joint. Cases have been described when the tendon passes through the cavity with its upper part joint, as a result of which the upper anterior wall of the latter appears to be somewhat weakened. The subscapularis muscle attaches to the humerus most anteriorly of all the other muscles that form the rotator cuff (infraspinatus, supraspinatus and teres minor).
The site of the brachial attachment of the subscapularis muscle is usually very painful with the chronic nature of myofasciitis. To examine the shoulder attachment of the muscle, the patient brings the shoulder to the body, trying to reach the back with the elbow, and turns the shoulder outward. With this movement of the shoulder, the area of attachment of the subscapularis muscle to the humerus moves forward from under the humeral process and becomes accessible for palpation. The synovial subscapularis bursa, communicating with the cavity of the shoulder joint, separates the neck of the scapula from the subscapularis muscle. Innervation n. subscapularis (C 5-C 7). Blood supply a. Subscapularis.
Course and topography m . subscapularis
The subscapularis muscle rotates the shoulder inward (pronates) and brings it to the body, and also, together with other muscles, holds the head of the humerus in the glenoid cavity. Since the deltoid muscle is attached proximal to the middle of the shoulder, when the shoulder is abducted, it pulls the head of the humerus upward from the glenoid cavity to brachial process, but the subscapularis muscle counteracts this displacement of the head.
An idea of the nature of the actions of the subscapularis muscle will help to understand the mechanism of dysfunction of the hand that occurs with pathology of the subscapularis muscle. A pathological process in the subscapularis muscle can lead to severe shortening of this muscle, as a result of which the muscle holds the shoulder in an inwardly rotated position and a person cannot fully supinate the hand with the arm straightened due to limited outward rotation of the shoulder.
Damage to the subscapularis muscle causes severe pain, both at rest and with movement. The area of main pain is in the posterior projection of the shoulder joint, but can spread down the posterior region of the shoulder to the elbow. Some patients experience referred pain and tenderness in the form of a cuff surrounding the wrist, which has diagnostic significance, and on the dorsum of the wrist the pain and tenderness are more pronounced than on its palmar side. Due to pain in the wrist, patients wear the watch on the other hand. In the early stages of subscapularis disease, patients can lift their arm up and forward, but they cannot throw their arm back when, for example, trying to throw a ball. According to TravellJ . G ., the appearance of a focus of tension in the subscapularis muscle leads to a gradual increase in limited mobility in the joint due to pain, which causes damage to the pectoralis major and minor, teres major, latissimus, triceps and, finally, deltoid muscles. Ultimately, all muscles can be affected shoulder girdle. From this moment on, none of the affected muscles can be stretched to their full length, and all movements in the shoulder joint are severely limited. The shoulder joint becomes "frozen" , and after this, trophic disorders often appear. However, it should be noted that the term “frozen shoulder” is interpreted differently in the literature, numerous reasons for the development of restriction of movement in the shoulder joint are given, and a variety of clinical symptoms of this disease are given.
Knowledge of the topographic anatomy of the subscapularis muscle makes it clear that an isolated lesion of this muscle limits mobility in the shoulder joint, but does not impair the movement of the scapula relative to the chest. Therefore, when examining a patient whose shoulder movement is limited, the mobility of the scapula should first be checked. For this purpose, the doctor places his palm on the patient’s shoulder blade and invites him to move his hand away. If, in addition to limited mobility in the shoulder joint, the mobility of the scapula is limited, then pathology of the pectoralis minor, serratus anterior, trapezius and rhomboid muscles should be suspected.
IMPINGMENT SYNDROME. When raising the arm, even normally, there is a slight compression of the tendons between the head of the humerus and the acromion.
If the space between the acromion and the rotator cuff tendons narrows, impingement syndrome occurs, which involves injury to the rotator cuff muscles. In the early stages of impingement syndrome, the main complaint of patients is diffuse, dull pain in the shoulder. The pain intensifies when you raise your arm up. Many patients report that the pain prevents them from falling asleep, especially if they lie on the side of the affected shoulder joint.
A pathognomonic symptom of impingement syndrome is the occurrence of acute pain in the patient when trying to reach the back pocket of his trousers or unfasten his bra. In later stages, the pain intensifies, possibly causing joint stiffness.
Sometimes there is a clicking sound in the joint when the arm is lowered. Weakness and difficulty raising your arm may indicate a rotator cuff tear.
Relationship between the acromion and rotator cuff muscles during arm elevation

Thus, the clinical picture of impingement syndrome consists of manifestations inherent in damage to the muscles that make up the rotator cuff.
Contents of the article: classList.toggle()">toggle
Physiotherapeutic treatment
The goal of physiotherapy is to improve blood flow and circulation, stimulate metabolic processes and restoration in tissues. The following procedures are prescribed:
- Electromagnetic therapy;
- Infrared irradiation;
- Iontophoresis;
- Ultrasound;
- Ozokerite;
- Laser therapy in a stimulating dose.
It is highly desirable for recovery after a fracture of the tubercle of the humerus to undergo sanatorium treatment, which uses balneotherapy (mineral baths) and peloidotherapy (mineral mud), thalassotherapy (sea bathing).
Therapeutic massage
Massage has excellent restorative properties. It normalizes blood circulation and metabolism, eliminates muscle contractures and increases their contractility, promotes the resorption of edema of congestion in the joint and limb.
Massage is prescribed immediately after immobilization is removed provided that the skin is free of abrasions, bedsores, diaper rash and other damage. The basic rules of massage are:

Massage is indicated not only for the entire limb, but also for the shoulder girdle, collar area and even the back. It can be done throughout the entire rehabilitation for 10-15 sessions with breaks.
Possible complications of a fracture and their prevention
With a fracture of the greater tubercle of the shoulder, the most common complications are:
- Damage to the long head of the biceps brachii muscle (biceps). Damage occurs at the moment of injury. The muscle fibers pass in the groove between the greater and lesser tubercles of the shoulder and in case of displaced fractures they are injured by fragments. Treatment is surgical (suturing the muscle);
- Non-union of the tubercle and its fragments occurs due to insufficient reposition or poor fixation of the limb. In this case, the function cannot be restored, so surgical treatment is metal osteosynthesis;
- The formation of myositis ossificans is the deposition of calcium, ossification of muscle fibers attached to the tubercle. Treatment is surgical; in the initial stage, it can be eliminated with laser therapy;
- Development of post-traumatic arthrosis and contracture of the shoulder joint. Arthrosis of the shoulder joint is damage to cartilage tissue, bone growths, this is always the result of insufficient rehabilitation. It is treated conservatively, prevention consists of professional rehabilitation treatment after a fracture.
A fracture of the greater tuberosity of the humerus is uncommon, but can cause many problems.. Timely professional treatment and high-quality rehabilitation will ensure complete restoration of joint function and quality of life.
Anatomically, the humerus is part of the upper limb - from the elbow to the shoulder joint. Knowing where each of its elements is located is useful for the overall development and understanding of the mechanics of the human body. The structure, development, and possible injuries of this critical structure are described below.
When studying the structure of the humerus, we distinguish: the central part of the body (diaphysis), proximal (upper) and distal (lower) epiphyses, where ossification (ossification) occurs last, metaphyses, small epiphyseal tubercles - apophyses.
On the upper epiphysis there is a weakly defined anatomical neck, which passes into the head of the humerus. The lateral part of the pommel of the bone is marked by a large tubercle - one of the apophyses to which the muscles are attached. In front of the upper epiphysis there is a small tubercle that performs the same function. Between the proximal end of the bone and the body, the surgical neck of the humerus stands out, which is especially vulnerable to injury due to a sharp change in the cross-sectional area.
The cross-section changes from one epiphysis to another. Round at the upper epiphysis, towards the lower it becomes triangular. The body of the bone is relatively smooth; an intertubercular groove begins on its anterior surface near the head. It is located between the two apophyses and spirally deviates to the medial side. Almost in the middle of the height of the bone, somewhat closer to the upper part, a smoothed deltoid tuberosity protrudes - the place of attachment of the corresponding muscle. In the trilateral area near the distal epiphysis, posterior and anterior edges are distinguished - medial and lateral.
The distal epiphysis has a complex shape. On the sides there are protrusions - condyles (internal and external), easily detectable by touch. Between them there is a so-called block - a formation of a complex shape. In front there is a spherical capitate elevation. These parts have evolved to contact the radius and ulna bones. The epicondyles are protrusions on the condyles that are used to attach muscle tissue.
The upper epiphysis together with the scapular cavity make up a spherical and extremely mobile shoulder joint, responsible for the rotational movements of the arm. The upper limb carries out actions within approximately a hemisphere, in which it is assisted by the bones of the shoulder girdle - the collarbone and scapula.
The distal epiphysis is part of the complex elbow joint. The connection of the shoulder lever with the two bones of the forearm (radius and ulna) forms two of the three simple joints of this system - the humeroulnar and humeroradial joints. In this area, flexion-extension movements and slight rotation of the forearm relative to the shoulder are possible.
Functions
The humerus is essentially a lever. Anatomy predetermines its active participation in the movements of the upper limb, increasing their range. Partially when walking, it compensates for the periodic shift of the body’s center of gravity to maintain balance. It can play a supporting role and take on part of the load while climbing flights of stairs, playing sports, and in certain body positions. Most of the movements involve the forearm and shoulder girdle.
Development
Ossification of this cartilage structure is completed only upon reaching 20-23 years of age. Anatomy studies performed using x-rays show the following picture of ossification of the shoulder.
- The point of the medial region of the head of the humerus originates in the womb or in the first year of life.
- The lateral part of the upper epiphysis and the greater apophysis acquire their own ossification centers by 2-3 years.
- The lesser tubercle is one of the rudiments of osteogenesis of the humerus and begins to harden at the age of 3 to 4 years in young children.
- At about 4-6 years the head becomes completely ossified.
- By the age of 20-23, osteogenesis of the humerus is completed.
Damage
The mobility of the shoulder joints explains the frequency of injury to individual areas of the shoulder. Fractures of bone formations can occur when exposed to significant force. The surgical neck of the bone often suffers, being an area of stress concentration due to mechanical stress. Joint pain can signal a variety of problems. For example, glenohumeral periarthritis - inflammation of the shoulder joint - can be considered as a likely sign of neck osteochondrosis.
The displacement of bones in a joint relative to each other, which is not eliminated due to the elasticity of the supporting tissues, is called a dislocation. It is not always possible to differentiate a dislocation from a fracture without medical equipment. This phenomenon may be accompanied by a fracture of the humeral neck or breaking off of the greater tubercle. Reducing a dislocation on your own, without the appropriate knowledge and experience, is strictly not recommended.









