What is cardiogenic shock, emergency care for the victim. Cardiogenic shock Cardiogenic shock ICD
Cardiogenic shock is characterized by a sustained drop in blood pressure. The upper pressure drops below 90 mmHg. In most cases, this situation occurs as a complication of myocardial infarction and one should be prepared for its occurrence in order to help the core.
The occurrence of cardiogenic shock is facilitated (especially of the left ventricular type), in which many myocardial cells suffer. The pumping function of the heart muscle (especially the left ventricle) is impaired. As a result, problems begin in target organs.
First of all, the kidneys (the skin clearly turns pale and its humidity increases), the central nervous system, and pulmonary edema occur. Prolonged persistence of a state of shock invariably leads to the death of the core.
Due to its importance, cardiogenic shock ICD 10 is allocated to a separate section - R57.0.
Cardiogenic shock is a life-threatening condition characterized by a significant decrease in blood pressure (arterial hypotension should last at least thirty minutes) and severe tissue and organ ischemia as a result of hypoperfusion (insufficient blood supply). As a rule, shock is combined with cardiogenic pulmonary edema.
Attention. True cardiogenic shock is the most dangerous manifestation of AHF (acute heart failure) of the left ventricular type, caused by severe myocardial damage. The probability of death with this condition ranges from 90 to 95%.
Cardiogenic shock - causes
More than eighty percent of all cases of cardiogenic shock are a significant decrease in blood pressure during myocardial infarction (MI) with severe damage to the left ventricle (LV). To confirm the occurrence of cardiogenic shock, more than forty percent of the LV myocardial volume must be damaged.
Much less frequently (about 20%), cardiogenic shock develops due to acute mechanical complications of MI:
- acute mitral valve insufficiency due to rupture of the papillary muscles;
- complete separation of the papillary muscles;
- myocardial ruptures with the formation of an IVS defect (interventricular septum);
- complete rupture of the IVS;
- cardiac tamponade;
- isolated right ventricular myocardial infarction;
- acute cardiac aneurysm or pseudoaneurysm;
- hypovolemia and a sharp decrease in cardiac preload.

The incidence of cardiogenic shock in patients with acute MI ranges from 5 to 8%.
Risk factors for the development of this complication are considered:
- anterior localization of the infarction,
- the patient has a history of heart attacks,
- old age of the patient,
- presence of underlying diseases:
- diabetes mellitus,
- chronic renal failure,
- severe arrhythmias,
- chronic heart failure,
- LV systolic dysfunction (left ventricle),
- cardiomyopathy, etc.
Types of cardiogenic shock
Cardiogenic shock can be:- true;
- reflex (development of pain collapse);
- arrhythmogenic;
- Areactive.

True cardiogenic shock. Pathogenesis of development
 For the development of true cardiogenic shock, the death of more than 40% of the LV myocardial cells is necessary. In this case, the remaining 60% should start working at double load. The critical decrease in systemic blood flow that occurs immediately after a coronary attack stimulates the development of reciprocal, compensatory reactions.
For the development of true cardiogenic shock, the death of more than 40% of the LV myocardial cells is necessary. In this case, the remaining 60% should start working at double load. The critical decrease in systemic blood flow that occurs immediately after a coronary attack stimulates the development of reciprocal, compensatory reactions.
Due to the activation of the sympathoadrenal system, as well as the action of glucocorticosteroid hormones and the renin-angiotensin-aldosterone system, the body tries to increase blood pressure. Thanks to this, in the first stages of cardiogenic shock, blood supply to the coronary system is maintained.
However, activation of the sympathoadrenal system leads to the appearance of tachycardia, increased contractile activity of the heart muscle, increased oxygen demand of the myocardium, spasm of microcirculatory vessels and increased cardiac afterload.
The occurrence of generalized microvascular spasm enhances blood clotting and creates a favorable background for the occurrence of DIC syndrome.
Important. Severe pain associated with severe damage to the heart muscle also aggravates existing hemodynamic disorders.
As a result of impaired blood supply, renal blood flow decreases and renal failure develops. Fluid retention by the body leads to an increase in circulating blood volume and an increase in cardiac preload.
RCHR (Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical protocols of the Ministry of Health of the Republic of Kazakhstan - 2016
Cardiogenic shock (R57.0)
Emergency medicine
General information
Brief description
Approved
Joint Commission on Healthcare Quality
Ministry of Health and Social Development of the Republic of Kazakhstan
dated November 29, 2016
Protocol No. 16
TOardiogenic shock- a life-threatening condition of critical organ hypoperfusion, due to a decrease in cardiac output, which is characterized by:
- Decrease in SBP<90 мм.рт.ст. в течение более 30 минут, среднего АД менее 65 мм рт.ст. в течение более 30 мин, либо необходимости применения вазопрессоров для поддержания САД≥90 мм.рт.ст.;
- Signs of pulmonary congestion or increased left ventricular filling pressure;
- Signs of organ hypoperfusion, at least the presence of one of the following criteria:
· disturbance of consciousness;
· cold damp skin;
· oliguria;
· increase in plasma serum lactate > 2 mmol/l.
Correlation of ICD-10 and ICD-9 codes
| ICD-10 | ICD-9 | ||
| Code | Name | Code | Name |
| R57.0 | Cardiogenic shock | - | - |
Date of protocol development/revision: 2016
Protocol users: cardiologists, resuscitators, interventionalists
cardiologists/x-ray surgeons, cardiac surgeons, therapists, general practitioners, emergency doctors and paramedics, doctors of other specialties.
Level of evidence scale:
| Recommendation classes | Definition |
Proposed wording |
| Class I | Data and/or general agreement that a particular treatment or intervention useful, effective, have advantages. | Recommended/shown |
| Class II | Conflicting data and/or differences of opinion about the benefits/effectiveness specific treatment or procedure. | |
| Class IIa | Most data/opinion says about the benefits/efficiency. |
It is advisable Apply |
| Class IIb | Data/opinion is not so convincing about the benefits/efficiency. | Can be used |
| Class III | Evidence and/or general agreement that a particular treatment or intervention is not beneficial or effective and, in some cases, may be harmful. | Not recommended |
Classification
Classification:
Due to development:
· ischemic origin (acute myocardial infarction) - (80%).
· mechanical origin during AMI (rupture of the interventricular septum (4%) or free wall (2%), acute severe mitral regurgitation (7%).
· mechanical origin in other conditions (decompensated valvular heart disease, hypertrophic cardiomyopathy, cardiac tamponade, outflow tract obstruction, trauma, tumors, etc.).
· myogenic genesis (myocarditis, cardiomyopathies, cytotoxic agents, etc.).
· arrhythmogenic genesis (tachy-bradyarrhythmia).
Acute right ventricular failure.
In 2/3 of cases, the clinical picture of shock is absent upon admission and develops within 48 hours after the clinical picture of myocardial infarction develops.
Diagnostics (outpatient clinic)
OUTPATIENT DIAGNOSTICS
Diagnostic criteria:
- decrease in SBP< 90 мм.рт.ст. в течение более 30 минут, среднего АД менее 65 мм рт.ст. в течение более 30 мин, либо необходимости применения вазопрессоров для поддержания САД ≥90 мм.рт.ст.;
· disturbance of consciousness;
· cold damp skin;
· oliguria;
· increase in plasma serum lactate > 2 mmol/l (1.2).
Complaints
· age >65 years;
· Heart rate above 75 beats/min.;
· MI of anterior localization.
Physical examination: draws attention to the presence of signs of peripheral hypoperfusion:
gray cyanosis or pale cyanotic, “marbled”, moist skin;
acrocyanosis;
collapsed veins;
cold hands and feet;
nail bed test for more than 2 s. (decreased peripheral blood flow velocity).
Impaired consciousness: lethargy, confusion, less often - agitation. Oliguria (decrease in urine output less than<0,5 мл/кг/ч). Снижение систолического артериального давления менее 90 мм.рт.ст.; снижение пульсового артериального давления до 20 мм.рт.ст. и ниже., снижение среднего АД менее 65 мм рт.ст. (формула расчета среднего АД = (2ДАД + САД)/3).
Laboratory tests at the prehospital stage: not provided.
.
1. ECG diagnostics- possible signs of ACS, paroxysmal rhythm disturbances, conduction disturbances, signs of structural heart damage, electrolyte disturbances (see relevant protocols).
2. Pulse oximetry.
Diagnostic algorithm:
Diagnostic algorithm for cardiogenic shock at the prehospital stage.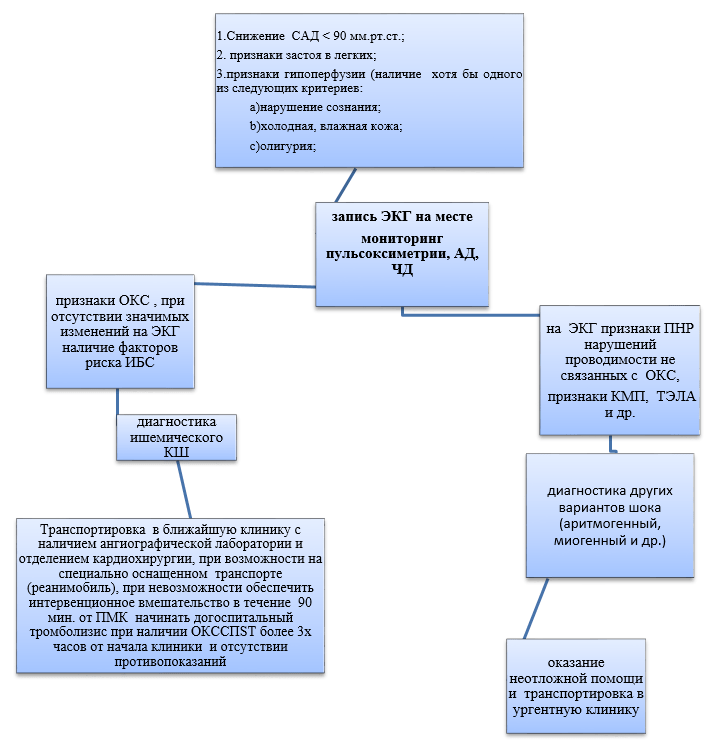
The patient must be transported to centers with 24-hour interventional and cardiac surgery services with the possibility of using circulatory support devices. If this is not possible, delivery to the nearest urgent clinic with a cardiac intensive care unit.
Diagnostics (ambulance)
DIAGNOSTICS AT THE EMERGENCY CARE STAGE**
Diagnostic measures:
Definition of diagnostic criteria for CABG:
1.decrease in SBP< 90 мм.рт.ст. в течение более 30 минут, среднего АД менее 65 мм рт.ст. в течение более 30 мин, либо необходимости применения вазопрессоров для поддержания САД ≥ 90 мм.рт.ст.;
2. signs of pulmonary congestion or increased left ventricular filling pressure;
3. signs of organ hypoperfusion, at least the presence of one of the following criteria:
· disturbance of consciousness;
· cold damp skin;
· oliguria;
· increase in serum plasma lactate > 2 mmol/l (1.2).
Complaints: symptoms of ACS are possible (detailed in the relevant protocols) or signs of non-ischemic heart damage, along with the appearance of signs of acute hemodynamic failure and hypoperfusion: severe general weakness, dizziness, “fog before the eyes”, palpitations, a feeling of interruptions in the heart, suffocation.
Prognostic criteria for the development of ischemic cardiogenic shock:
· age >65 years,
· Heart rate above 75 beats/min,
a history of diabetes mellitus,
history of myocardial infarction, CABG,
presence of signs of heart failure upon admission,
· MI of anterior localization.
Physical examination: draws attention to the presence of signs of peripheral hypoperfusion: gray cyanosis or pale cyanotic, “marbled”, moist skin; acrocyanosis; collapsed veins; cold hands and feet; nail bed test more than 2s. (decreased peripheral blood flow velocity). Impaired consciousness: lethargy, confusion, less often - agitation. Oliguria (decrease in urine output less than<0,5 мл/кг/ч). Снижение систолического артериального давления менее 90 мм.рт.ст.; снижение пульсового артериального давления до 20 мм.рт.ст. и ниже., снижение среднего АД менее 65 мм рт.ст. (формула расчета среднего АД = (2ДАД + САД)/3).
Percussion: expansion of the left border of the heart; on auscultation, muffled heart sounds, arrhythmias, tachycardia, protodiastolic gallop rhythm (pathognomonic symptom of severe left ventricular failure).
Breathing is shallow and rapid. The most severe course of cardiogenic shock is characterized by the development of cardiac asthma and pulmonary edema, suffocation appears, bubbling breathing, and a disturbing cough with pink frothy sputum. When percussing the lungs, dullness of the percussion sound in the lower parts is determined. Crepitation and fine bubbling rales can also be heard here. As alveolar edema progresses, wheezing is heard over more than 50% of the lung surface.
Instrumental studies:.
· ECG diagnostics - possible signs of ACS, paroxysmal rhythm disturbances, conduction disturbances, signs of structural heart damage, electrolyte disturbances (see relevant protocols).
· Pulse oximetry.
Diagnostic algorithm for cardiogenic shock at the prehospital stage
If there is clinical shock that has developed without an obvious reason, it is necessary to suspect cardiogenic shock and take a standard ECG.
High diastolic pressure suggests decreased cardiac output.
The patient must be transported to centers with 24-hour interventional and cardiac surgery services with the possibility of using circulatory support devices. If this is not possible, delivery to the nearest urgent clinic with a cardiac intensive care unit.
Diagnostics (hospital)
DIAGNOSTICS AT THE INPATIENT LEVEL**
Diagnostic criteria:
- decrease in SBP< 90 мм.рт.ст. в течение более 30 минут, среднего АД менее 65 мм рт.ст. в течение более 30 мин, либо необходимости применения вазопрессоров для поддержания САД ≥90 мм.рт.ст.;
- signs of pulmonary congestion or increased left ventricular filling pressure;
- signs of organ hypoperfusion, at least the presence of one of the following criteria:
· disturbance of consciousness;
· cold damp skin;
· oliguria;
· increase in plasma serum lactate > 2 mmol/l) (1,2).
Complaints: possible symptoms of ACS (detailed in the relevant protocols) or signs of non-ischemic heart damage, along with this, the appearance of signs of acute hemodynamic failure and hypoperfusion: severe general weakness, dizziness, “fog before the eyes”, palpitations, a feeling of interruptions in the heart area, suffocation .
Prognostic criteria for the development of ischemic cardiogenic shock:
· age >65 years;
· Heart rate above 75 beats/min;
· history of diabetes mellitus;
· history of myocardial infarction, CABG;
· presence of signs of heart failure upon admission;
· MI of anterior localization.
Physical examination: Physical examination: pay attention to the presence of signs of peripheral hypoperfusion: gray cyanosis or pale cyanotic, “marbled”, moist skin; acrocyanosis; collapsed veins; cold hands and feet; nail bed test more than 2s. (decreased peripheral blood flow velocity). Impaired consciousness: lethargy, confusion, less often - agitation. Oliguria (decrease in urine output less than<0,5 мл/кг/ч). Снижение систолического артериального давления менее 90 мм.рт.ст.; снижение пульсового артериального давления до 20 мм.рт.ст. и ниже., снижение среднего АД менее 65 мм рт.ст. (формула расчета среднего АД = (2ДАД + САД)/3).
Percussion: expansion of the left border of the heart; on auscultation, muffled heart sounds, arrhythmias, tachycardia, protodiastolic gallop rhythm (pathognomonic symptom of severe left ventricular failure).
Breathing is shallow and rapid. The most severe course of cardiogenic shock is characterized by the development of cardiac asthma and pulmonary edema. There is suffocation, bubbling breathing, and a disturbing cough with pink, frothy sputum. When percussing the lungs, dullness of the percussion sound in the lower parts is determined. Crepitation and fine bubbling rales can also be heard here. As alveolar edema progresses, wheezing is heard over more than 50% of the lung surface.
Laboratory criteria:
· increase in plasma lactate (in the absence of epinephrine therapy) > 2 mmol/l;
· increased BNP or NT-proBNP>100 pg/mL, NT-proBNP>300 pg/mL, MR-pro BNP>120 pg/mL;
metabolic acidosis (pH<7.35);
Increased level of creatinine in blood plasma;
· partial pressure of oxygen (PaO2) in arterial blood<80 мм рт.ст. (<10,67 кПа), парциальное давление CO2 (PCO2) в артериальной крови>45 mmHg (> 6 kPa).
Instrumental criteria:
· Pulse oximetry - decrease in oxygen saturation (SaO2)<90%. Однако необходимо помнить, что нормальный показатель сатурации кислорода не исключает гипоксемию.
· X-ray of the lungs - signs of left ventricular failure.
· ECG diagnostics - signs of ACS, paroxysmal rhythm disturbances, conduction disturbances, signs of structural heart damage, electrolyte disturbances (see relevant protocols).
· Catheterization of the superior vena cava for periodic or continuous monitoring of venous blood oxygen saturation (ScvO2).
· Echocardiography (transthoracic and/or transesophageal) should be used to identify the cause of cardiogenic shock, for subsequent hemodynamic evaluation, and to identify and treat complications.
· Emergency coronary angiography followed by coronary revascularization with angioplasty or, in exceptional cases, CABG, is required for ischemic cardiogenic shock, regardless of the time since the onset of pain.
There is no need to monitor central venous pressure due to limitations as a marker of pre- and afterload.
Diagnostic algorithm for the development of a CABG clinic at the inpatient stage

List of basic diagnostic measures
general blood test;
general urine analysis;
· biochemical blood test (urea, creatinine, ALT, AST, blood bilirubin, potassium, sodium);
· blood sugar;
· cardiac troponins I or T;
arterial blood gases;
· plasma lactate (in the absence of epinephrine therapy);
· BNP or NT-proBNP (if available).
List of additional diagnostic measures:
· Thyroid-stimulating hormone.
· Procalcitonin.
· INR.
· D-dimer.
· In case of cardiogenic shock refractory to empirical therapy, it is necessary to monitor cardiac output, mixed venous blood saturation (SvO2) and central venous blood (ScvO2).
· Pulmonary artery catheterization may be performed in patients with refractory cardiogenic shock and right ventricular dysfunction.
· Transpulmonary thermodilution and study of venous (SvO2) and central (ScvO2) venous saturation parameters can be performed in case of cardiogenic shock refractory to initial therapy, caused primarily by right ventricular dysfunction.
· Arterial catheterization may be performed to monitor diastolic blood pressure, the pressure fluctuation during ventricular contraction.
· Contrast-enhanced CT or MSCT to exclude PE as a cause of shock.
Differential diagnosis
Differential diagnosis and rationale for additional studies
| Diagnosis | Rationale for differential diagnosis | Surveys | Diagnosis exclusion criteria |
| Aortic dissection |
- Pain syndrome -Arterial hypotension |
- ECG in 12 leads |
. The pain is very intense, often wave-like. . The onset is lightning fast, often against the background of arterial hypertension or during physical or emotional stress; presence of neurological symptoms. . The duration of pain ranges from several minutes to several days. . The pain is localized in the retrosternal region with irradiation along the spine and along the branches of the aorta (to the neck, ears, back, abdomen). . Absent or decreased pulse |
| TELA |
- Pain syndrome -Arterial hypotension |
- ECG in 12 leads |
. Shortness of breath or worsening chronic shortness of breath (RR greater than 24/min) . Cough, hemoptysis, pleural friction rub . Presence of risk factors for venous thromboembolism |
| Vasovagal syncope |
-Arterial hypotension - lack of consciousness |
ECG in 12 leads |
. usually triggered by fear stress or pain. .Most common among healthy young people |
Treatment abroad
Get treatment in Korea, Israel, Germany, USA
Get advice on medical tourism
Treatment
Drugs (active ingredients) used in treatment
Groups of drugs according to ATC used in treatment
Treatment (outpatient clinic)
OUTPATIENT TREATMENT
Treatment tactics.
Non-drug treatment: not provided.
Drug treatment (see Appendix 1):
Fluid infusion (NaCl or Ringer's solution >200ml/15-30min) is recommended as first-line therapy in the absence of signs of hypervolemia .
Ringer's solution
:
· Dopamine (ampoules 0.5% or 4%, 5 ml) inotropic dose of dopamine - 3-5 mg/kg/min; vasopressor dose >
Algorithm of therapeutic actions for cardiogenic shock at the prehospital stage.

1. In the absence of signs of pulmonary edema or right ventricular overload, careful volume replacement with fluid is necessary.
2. At the prehospital stage, norepinephrine is the vasopressor of choice.
3. Non-invasive ventilation is carried out only in the presence of a clinical diagnosis of respiratory distress syndrome.
4. The patient must be transported to centers with 24-hour interventional and cardiac surgery services with the possibility of using circulatory support devices. If this is not possible, delivery to the nearest urgent clinic with a cardiac intensive care unit.
Other types of pre-hospital treatment:
· oxygen therapy - < 90%);
· non-invasive ventilation - performed in patients with respiratory distress syndrome (RR >25/min, SpO2<90%);
· electropulse therapy
Modern research did not reveal effectiveness placing the patient in the Trendelenburg position (horizontal position with the leg end elevated) to sustainably improve cardiac output and increase blood pressure.
Indications for consultation with specialists at this stage not provided.
Preventive measures - maintaining basic hemodynamic parameters.
Monitoring the patient's condition at the prehospital stage:
Non-invasive monitoring:
· pulse oximetry;
· blood pressure measurement;
· measurement of respiratory rate;
· assessment of the electrocardiogram. An ECG should be recorded within the first minute of contact with the patient and again in the ambulance.
relief of symptoms;
preventing heart and kidney damage.
Treatment (ambulance)
TREATMENT AT THE EMERGENCY STAGE**
Drug treatment (see Appendix 1):
Fluid infusion (NaCl or Ringer's solution > .
· Dobutamine and levosimendan are used for inotropic purposes (to increase cardiac output) (the use of levosimendan is especially indicated for the development of CABG in patients with CHF taking β-blockers). Dobutamine infusion is carried out at a dose of 2-20 mg/kg/min. Levosimendan can be administered at a dose of 12 mcg/kg over 10 minutes, followed by an infusion of 0.1 mg/kg/min, with the dose reduced to 0.05 or increased if ineffective to 0.2 mg/kg/min. It is important that the heart rate does not exceed 100 beats/min. If tachycardia or cardiac arrhythmias develop, the dose of inotropes should be reduced if possible.
· Vasopressors should be used only if it is impossible to achieve target SBP values and eliminate symptoms of hypoperfusion during therapy with infusion solutions and dobutamine/levosimendan.
· The vasopressor of choice should be norepinephrine. Norepinephrine is administered at a dose of 0.2-1.0 mg/kg/min.
· Loop diuretics - used cautiously when clinical cardiogenic shock is combined with acute left ventricular failure, only against the background of normalization of blood pressure numbers. The initial dose of a loop diuretic bolus is 20-40 mg.
· Drug treatment depending on the cause of CABG (ACS, paroxysmal arrhythmias, and other conditions according to protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan).
List of essential medicines:
· Dobutamine* (bottle 20 ml, 250 mg; ampoules 5% 5 (infusion concentrate).
· Norepinephrine hydrotartrate* (ampoules 0.2% 1 ml)
· Saline solution 0.9% solution 500 ml
Ringer's solution
For the rest of the main medications, see the relevant diagnostic and treatment protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan (ACS, paroxysmal arrhythmias, and other conditions)
List of additional medicines:
Levosimendan (2.5 mg/ml, 5 ml vial)
· Dopamine (ampoules 0.5% or 4%, 5 ml) inotropic dose of dopamine - 3-5 mg/kg/min; vasopressor dose >5 mg/kg/min (only in the absence of dobutamine, as according to updated recommendations it is not recommended for use in cardiogenic shock.
· Adrenaline hydrochloride (ampoules 0.1% 1 ml) if norepinephrine is ineffective. A bolus of 1 mg is administered intravenously. during resuscitation, repeated administration every 3-5 minutes. Infusion 0.05-0.5 mg/kg/min.
· Furosemide - 2 ml (ampoule) contains 20 mg - in the presence of clinical signs of pulmonary edema, after eliminating severe hypotension.
· Morphine (solution for injection in an ampoule of 1%, 1.0 ml) in the presence of pain, agitation and severe shortness of breath.
For other additional medications, see the relevant diagnostic and treatment protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan (ACS, paroxysmal arrhythmias, and other conditions).
Algorithm of therapeutic actions for cardiogenic shock at the prehospital stage

In the absence of signs of pulmonary edema or right ventricular overload, careful volume replacement with fluid is necessary.
- In the prehospital stage, norepinephrine is the vasopressor of choice.
- Non-invasive ventilation is carried out only in the presence of a clinical diagnosis of respiratory distress syndrome.
- The patient must be taken to centers with 24-hour interventional and cardiac surgery services with the possibility of using circulatory support devices. If this is not possible, delivery to the nearest urgent clinic with a cardiac intensive care unit.
Treatment (inpatient)
INPATIENT TREATMENT**
Treatment tactics
Non-drug treatment: not provided.
Drug treatment(See Appendix 1.) :
Fluid infusion (NaCl or Ringer's solution >200 ml/15-30 min) is recommended as first-line therapy in the absence of signs of hypervolemia .
· Dobutamine and levosimendan are used for inotropic purposes (to increase cardiac output) (the use of levosimendan is especially indicated for the development of CABG in patients with CHF taking β-blockers). Dobutamine infusion is carried out at a dose of 2-20 mg/kg/min. Levosimendan can be administered at a dose of 12 mcg/kg over 10 minutes, followed by an infusion of 0.1 mg/kg/min, with the dose reduced to 0.05 or increased if ineffective to 0.2 mg/kg/min. It is important that the heart rate does not exceed 100 beats/min. If tachycardia or cardiac arrhythmias develop, the dose of inotropes should be reduced if possible.
· Vasopressors should be used only if it is impossible to achieve target SBP values and eliminate symptoms of hypoperfusion during therapy with infusion solutions and dobutamine/levosimendan. The vasopressor of choice should be norepinephrine. Norepinephrine is administered at a dose of 0.2-1.0 mg/kg/min.
· Loop diuretics - used cautiously when clinical cardiogenic shock is combined with acute left ventricular failure, only against the background of normalization of blood pressure numbers. The initial dose of a loop diuretic bolus is 20-40 mg.
· Prevention of thromboembolic complications with heparin or other anticoagulants in the absence of contraindications.
· Drug treatment depending on the cause of CABG (ACS/AMI, paroxysmal arrhythmias, and other conditions according to protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan).
List of essential medicines:
· Dobutamine* (20 ml bottle, 250 mg; ampoules 5% 5 (infusion concentrate)
· Norepinephrine hydrotartrate* (ampoules 0.2% 1 ml)
· Saline solution 0.9% solution 500 ml
Ringer's solution
Fondaparinux (0.5ml 2.5 mg)
Enoxaparin sodium (0.2 and 0.4 ml)
· UFH (5000 IU)
For the rest of the main medications, see the relevant diagnostic and treatment protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan (ACS, paroxysmal arrhythmias, and other conditions)
List of additional medicines:
Levosimendan (2.5 mg/ml, 5 ml vial)
· Dopamine (ampoules 0.5% or 4%, 5 ml) inotropic dose of dopamine - 3-5 mg/kg/min; vasopressor dose >5 mg/kg/min (only in the absence of dobutamine, as according to updated recommendations it is not recommended for use in cardiogenic shock.
· Adrenaline hydrochloride (ampoules 0.1% 1 ml) if norepinephrine is ineffective. A bolus of 1 mg is administered intravenously. during resuscitation, repeated administration every 3-5 minutes. Infusion 0.05-0.5 mg/kg/min.
· Furosemide - 2 ml (ampoule) contains 20 mg - in the presence of clinical signs of pulmonary edema, after eliminating severe hypotension.
· Morphine (solution for injection in an ampoule of 1%, 1.0 ml) in the presence of pain, agitation and severe shortness of breath.
For other additional medications, see the relevant diagnostic and treatment protocols approved by the ES of the Ministry of Health of the Republic of Kazakhstan (ACS, paroxysmal arrhythmias, and other conditions)
Monitoring blood pressure and cardiac outputin the intensive care unit for CABG
· An average blood pressure of at least 65 mm Hg must be achieved. Art. with inotropic treatment or vasopressors or higher if there is a history of hypertension. The target mean arterial pressure should be adjusted to 65-70 mmHg. Hg Art., since higher numbers do not affect the outcome, except for patients with a history of arterial hypertension.
· In a patient without bradycardia, low DBP is usually associated with a fall in arterial tone and requires the use of vasopressors or an increase in their dosage if the mean arterial pressure<65 мм. рт.
· In cardiogenic shock, norepinephrine should be used to restore perfusion pressure.
· Epinephrine may be a therapeutic alternative to the combination of dobutamine and norepinephrine, but it is associated with a greater risk of arrhythmia, tachycardia, and hyperlactatemia.
· Dobutamine in cardiogenic shock should be used to treat low cardiac output. Dobutamine should be used at the lowest possible dose, starting at 2 mcg/kg/min. Titration should be based on cardiac index and venous blood saturation (SvO2). Dopamine should not be used in cardiogenic shock.
· Phosphodiesterase inhibitors or levosimendan should not be used as first-line drugs. However, these classes of drugs, and in particular levosimendan, may improve the hemodynamics of patients with cardiogenic shock refractory to catecholamines. There is a pharmacological rationale for using this strategy in patients chronically taking beta blockers. Perfusion of phosphodiesterase inhibitors or levosimendan improves hemodynamic parameters, but only levosimendan appears to improve prognosis. In cardiogenic shock refractory to catecholamines, the use of circulatory support should be considered rather than increasing pharmacological support.
Diagnostic and treatment algorithm for ischemic cardiogenic shock at the inpatient stage.

Surgical intervention:
1. Emergency revascularization PCI or CABG is recommended for cardiogenic shock caused by ACS, regardless of the time of onset of the clinical coronary event.
2. In case of cardiogenic shock caused by the presence of severe aortic stenosis, valvuloplasty is likely to be performed, if necessary, using ECMO.
3. Transcatheter aortic valve implantation is currently contraindicated in patients with CABG.
4. In case of cardiogenic shock caused by severe aortic or mitral insufficiency, cardiac surgery should be performed immediately.
5. For cardiogenic shock due to mitral valve regurgitation, intra-aortic balloon pump and vasoactive/inotropic drugs can be used to stabilize the condition pending surgery, which should be performed immediately (<12 ч).
6. If interventricular communication develops, the patient should be transferred to an expert center to discuss surgical treatment.
7. Milrinone or levosimendan can be used as an alternative to dobutamine as second-line therapy for cardiogenic shock after cardiac surgery. Levosimendan can be used as first-line therapy for CABG after coronary artery bypass grafting.
8. Levosimendan is the only drug for which a randomized trial showed a significant reduction in mortality when treated with post-CABG surgery compared with dobutamine.
9. Milrinone can be used as first-line therapy for inotropic effect in cardiogenic shock due to right ventricular failure.
10. Levosimendan may be used as first-line therapy for cardiogenic shock after surgery (weak agreement).
Other types of treatment:
- Oxygen therapy - in case of hypoxemia (arterial blood oxygen saturation (SaO2)< 90%).
- Non-invasive ventilation - performed in patients with respiratory distress syndrome (RR > 25/min, SpO2< 90%). Интубация рекомендуется, при выраженной дыхательной недостаточности с гипоксемией (РаО2< 60 мм рт.ст. (8,0 кПа), гиперкапнией (РаСО2 >50 mmHg (6.65 kPa) and acidosis (pH< 7,35), которое не может управляться неинвазивно.
- Electropulse therapy if there are signs of paroxysmal rhythm disturbances (see the corresponding protocol).
Current research has not shown that placing the patient in the Trendelenburg position (horizontal position with the leg end elevated) is effective in consistently improving cardiac output and blood pressure.
1. Routine use of intra-aortic balloon counterpulsation for CABG is not recommended.
2. Methods of assisted circulation in patients with CABG can be used for a short time, and indications for their use are determined by the patient’s age, his neurological status and the presence of concomitant pathology.
3. If temporary circulatory support is required, the use of peripheral extracorporeal membrane oxygenation is preferable.
4. The Impella® 5.0 device can be used in the treatment of myocardial infarction complicated by cardiogenic shock if the surgical team is experienced in its placement. However, the Impella® 2.5 device is not recommended for circulatory support during cardiogenic shock.
5. When transporting a patient with cardiogenic shock to a high-level center, it is recommended to create a mobile circulatory support device by installing veno-arterial ECMO.
Recommendations for general CABG:
1. In patients with cardiogenic shock and arrhythmia (atrial fibrillation), it is necessary to restore sinus rhythm, or slow down the heart rate if restoration is ineffective.
2. In case of cardiogenic shock, antithrombotic drugs should be used in the usual dose, but keep in mind that the hemorrhagic risk is higher in this situation. The only exception is that antiplatelet agents such as clopidogrel or ticagrelor should only be prescribed after surgical complications have been ruled out, i.e. not at the prehospital stage.
3. Nitrovasodilators should not be used in cardiogenic shock.
4. When cardiogenic shock is combined with pulmonary edema, diuretics can be used.
5. Beta blockers are contraindicated in cardiogenic shock.
6. In ischemic cardiogenic shock, it is recommended to maintain the hemoglobin level at about 100 g/l in the acute phase.
7. With non-ischemic genesis of cardiogenic shock, the hemoglobin level can be maintained above 80 g/l.
Features of the management of patients with cardiogenic shock caused by the use of cardiotoxic drugs (6):
1. Knowledge of the mechanism of cause (hypovolemia, vasodilation, decreased contractility) is important for the choice of treatment. Emergency echocardiography is mandatory, followed by continuous measurement of cardiac output and SvO2.
2. It is necessary to differentiate between hypokinetic cardiogenic shock and vasoplegic (vasodilation). The latter can usually be treated with vasopressors (norepinephrine) and volume expansion. The possibility of mixed forms or vasoplegic forms progressing to hypokinesia should not be overlooked.
3. In the presence of cardiotoxic effects during the development of shock, emergency echocardiography is necessary to identify a hypokinetic state.
4. In case of cardiogenic shock due to the cardiotoxic effect of drugs (sodium channel blockers, calcium blockers, beta blockers), it is necessary to transfer the patient to an expert center with experience in working with ECMO, especially if echocardiography shows a hypokinetic state. In cases of refractory or rapidly progressive shock that has developed in a center without ECMO, the use of a mobile circulatory assist device is necessary. Ideally, ECMO should be performed before the onset of multi-organ damage (liver, kidney, RDSS) and in all cases, before cardiac arrest. Only isolated vasoplegic shock is not an indication for ECMO.
5. The use of dobutamine, norepinephrine or the use of epinephrine is necessary, taking into account possible side effects (lactic acidosis).
6. It is possible to use glucagon (for the toxic effects of beta-blockers), insulin therapy (for the effects of calcium antagonists), lipid emulsion (for the cardiotoxic effect of local fat-soluble anesthetics) in combination with vasopressors/inotropes agents.
7. Medical maintenance treatment should not be a delay in ECMO for refractory shock.
8. It is possible to administer a molar solution of sodium bicarbonate (in a dose of 100 to 250 ml up to a maximum total dose of 750 ml) for toxic shock with impaired intraventricular conduction (wide QRS complex), along with other types of treatment.
Features of management of patients with CABG as a complication of end-stage heart disease
1. Patients with severe chronic heart disease should be assessed for eligibility for heart transplantation.
2. ECMO is considered as first-line therapy in cases of progressive or refractory shock (persistent lactic acidosis, low cardiac output, high-dose catecholamines, renal and/or liver failure) and cardiac arrest in patients with chronic severe cardiac disease without any contraindications for transplantation hearts.
3. When a patient with decompensated heart failure is admitted to the center without circulatory support, it is necessary to use the circulatory support of a mobile unit to implement venous-arterial ECMO with subsequent transfer of the patient to an expert center.
Indications for specialist consultation: cardiologist, interventional cardiologist, arrhythmologist, cardiac surgeon and other specialists according to indications.
Indications for transfer to the intensive care unit:
Patients with clinical shock are treated in intensive care units until clinical shock is completely relieved.
Indicators of treatment effectiveness
Improvement of hemodynamic parameters and organ perfusion:
· achieving the target mean arterial pressure of 65-70 mmHg;
· restoration of oxygenation;
relief of symptoms;
· Prevent heart and kidney damage.
Further management of a patient who has undergone CABG:
- Once the acute phase of cardiogenic shock has been relieved, appropriate oral treatment for heart failure should be instituted under close monitoring.
- Immediately after discontinuation of vasopressor drugs, beta blockers, angiotensin-converting enzyme inhibitors/sartans and aldosterone antagonists should be prescribed to improve survival by reducing the risk of arrhythmias and the development of cardiac decompensation.
- Once shock has resolved, patient management should be in accordance with the latest recommendations for the treatment of chronic heart failure. Treatment should be started with minimal doses after discontinuation of vasopressors and gradually increased to optimal doses. If tolerance is poor, a return to vasopressors is possible.
Medical rehabilitation
rehabilitation measures provided depending on the cause of CABG (myocardial infarction, myocarditis, cardiomyopathies, etc. (see relevant protocols).
Hospitalization
INDICATIONS FOR HOSPITALIZATION WITH INDICATION OF THE TYPE OF HOSPITALIZATION**
Indications for planned hospitalization: No
Indications for emergency hospitalization:
cardiogenic shock clinic is an indication for emergency hospitalization.
Information
Sources and literature
- Minutes of meetings of the Joint Commission on the Quality of Medical Services of the Ministry of Health of the Republic of Kazakhstan, 2016
- Recommendations on pre-hospital and early hospital management of acute heart failure: a consensus paper from the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine (2015). European Heart Journaldoi:10.1093/eurheartj/ehv066. 2.Managementofcardiogenicshock. European Heart Journal (2015)36, 1223–1230doi:10.1093/eurheartj/ehv051. 3.Cardiogenic Shock Complicating Myocardial Infarction: An Updated Review. British Journal of Medicine & Medical Research 3(3): 622-653, 2013. 4.Current Concepts and New Trends in the Treatment of Cardiogenic Shock Complicating Acute Myocardial InfarctionThe Journal of Critical Care Medicine 2015;1(1):5-10 . 5.2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 6.Experts’ recommendations for the management of adult patients with cardiogenicshock. Levyetal.AnnalsofIntensiveCare (2015) 5:17 7.Shammas, A. & Clark, A. (2007).Trendelenburg Positioning to Treat Acute Hypotension: Helpful or Harmful? ClinicalNurseSpecialist. 21(4), 181-188. PMID: 17622805 8.2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). European Heart Journaldoi:10.1093/eurheartj/ehw128.
Information
Abbreviations used in the protocol
| AHL | angiography laboratory |
| HELL | blood pressure |
| CABG | coronary artery bypass grafting |
| VABK | intra-aortic balloon counterpulsation |
| DBP | diastolic blood pressure |
| IHD | coronary heart disease |
| THEM | myocardial infarction |
| KMP | cardiomyopathy |
| CBS | acid-base state |
| KS | cardiogenic shock |
| AMI | acute myocardial infarction |
| OKS | acute coronary syndrome |
| PMK | first medical contact |
| Poland | paroxysmal rhythm disturbances |
| GARDEN | systolic blood pressure |
| TELA | pulmonary embolism |
| CHF | chronic heart failure |
| BH | respiration rate |
| PCI | percutaneous intervention |
| Heart rate | heart rate |
| EIT | electropulse therapy |
| ECG | electrocardiography |
| ECMO | extracorporeal membrane oxygenation |
List of protocol developers:
1) Zhusupova Gulnar Kairbekovna - Doctor of Medical Sciences, JSC “Astana Medical University”, head of the Department of Internal Medicine, Faculty of Continuing Professional Development and Additional Education.
2) Abseitova Saule Raimbekovna - Doctor of Medical Sciences, Associate Professor, JSC National Scientific Medical Center, Chief Researcher, Chief Freelance Cardiologist of the Ministry of Health of the Republic of Kazakhstan.
3) Zagorulya Natalya Leonidovna - JSC Astana Medical University, Master of Medical Sciences, assistant at the Department of Internal Medicine No. 2.
4) Yukhnevich Ekaterina Aleksandrovna - Master of Medical Sciences, PhD, RSE at Karaganda State Medical University, clinical pharmacologist, assistant at the Department of Clinical Pharmacology and Evidence-Based Medicine.
Conflict of interest: absent.
List of reviewers:
- Kapyshev T.S. - Head of the Department of Resuscitation and Intensive Care of JSC National Scientific Cardiac Surgery Center.
- Lesbekov T.D. - Head of the Department of Cardiac Surgery 1 JSC National Scientific Cardiac Surgery Center.
- Aripov M.A. - Head of the Department of Interventional Cardiology of JSC National Scientific Cardiac Surgery Center.
Conditions for reviewing the protocol: review of the protocol 3 years after its publication and from the date of its entry into force or if new methods with a level of evidence are available.
Appendix 1
Choice of drug treatment in patients with AHF/CABG and ACS after initial therapy a

Attached files
Attention!
- By self-medicating, you can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" cannot and should not replace a face-to-face consultation with a doctor. Be sure to contact a medical facility if you have any illnesses or symptoms that concern you.
- The choice of medications and their dosage must be discussed with a specialist. Only a doctor can prescribe the right medicine and its dosage, taking into account the disease and condition of the patient’s body.
- The MedElement website and mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Directory" are exclusively information and reference resources. The information posted on this site should not be used to unauthorizedly change doctor's orders.
- The editors of MedElement are not responsible for any personal injury or property damage resulting from the use of this site.
RCHR (Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Archive - Clinical protocols of the Ministry of Health of the Republic of Kazakhstan - 2007 (Order No. 764)
Cardiogenic shock (R57.0)
General information
Brief description
Cardiogenic shock- extreme degree of left ventricular failure, characterized by a sharp decrease in myocardial contractility (a drop in stroke and cardiac output), which is not compensated by an increase in vascular resistance and leads to inadequate blood supply to all organs and tissues, primarily vital organs. When a critical amount of left ventricular myocardium is damaged, pump failure may be recognized clinically as pulmonary failure or systemic hypotension, or both. With severe pumping failure, pulmonary edema may develop. The combination of hypotension with pump failure and pulmonary edema is known as cardiogenic shock. Mortality ranges from 70 to 95%.
Protocol code: E-010 "Cardiogenic shock"
Profile: emergency medical care
ICD-10 codes:
R57.0 Cardiogenic shock
I50.0 Congestive heart failure
I50.1 Left ventricular failure
I50.9 Heart failure, unspecified
I51.1 Rupture of chordae tendons, not elsewhere classified
I51.2 Rupture of papillary muscle, not elsewhere classified
Classification
Classification by stream: true cardiogenic.
Risk factors and groups
1. Extensive transmural myocardial infarction.
2. Repeated myocardial infarctions, especially heart attacks with rhythm and conduction disturbances.
3. Zone of necrosis equal to or greater than 40% of the mass of the left ventricular myocardium.
4. Decline in myocardial contractile function.
5. Decreased pumping function of the heart as a result of the remodeling process that begins in the first hours and days after the onset of acute coronary occlusion.
6. Cardiac tamponade.
Diagnostics
Diagnostic criteria
True cardiogenic shock
The patient complains of severe general weakness, dizziness, “fog before the eyes,” palpitations, a feeling of interruptions in the heart area, chest pain, suffocation.
1. Symptoms of peripheral circulatory failure:
Gray cyanosis or pale cyanotic, “marbled”, moist skin;
Acrocyanosis;
Collapsed veins;
Cold hands and feet;
Nail bed test for more than 2 s (decreased peripheral blood flow velocity).
2. Impaired consciousness: lethargy, confusion, less often - agitation.
3. Oliguria (decrease in diuresis less than 20 mm/hour, in severe cases - anuria).
4. Decrease in systolic blood pressure to less than 90 - 80 mm Hg.
5. Decrease in pulse blood pressure to 20 mm Hg. and below.
Percussion: expansion of the left border of the heart; on auscultation, muffled heart sounds, arrhythmias, tachycardia, protodiastolic gallop rhythm (pathognomonic symptom of severe left ventricular failure). Breathing is shallow and rapid.
The most severe course of cardiogenic shock is characterized by the development of cardiac asthma and pulmonary edema. There is suffocation, bubbling breathing, and a disturbing cough with pink, frothy sputum. When percussing the lungs, dullness of the percussion sound in the lower parts is determined. Crepitation and fine bubbling rales can also be heard here. As alveolar edema progresses, wheezing is heard over more than 50% of the lung surface.
The diagnosis is based on identifying a decrease in systolic blood pressure of less than 90 mmHg, clinical signs of hypoperfusion (oliguria, mental dullness, pallor, sweating, tachycardia) and pulmonary failure.
A. Reflex shock(pain collapse) develops in the first hours of the disease, during a period of severe pain in the heart region due to a reflex drop in total peripheral vascular resistance.
1. Systolic blood pressure is about 70-80 mm Hg.
2. Peripheral circulatory failure - pallor, cold sweat.
3. Bradycardia is a pathognomonic symptom of this form of shock.
4. The duration of hypotension does not exceed 1-2 hours, the symptoms of shock disappear on their own or after pain relief.
5. Develops with limited myocardial infarction of the posteroinferior sections.
6. Extrasystoles, atrioventricular block, rhythm from the AV junction are characteristic.
7. The clinical picture of reflex cardiogenic shock corresponds to grade I of severity.
B. Arrhythmic shock
1. Tachysystolic (tachyarrhythmic variant of cardiogenic shock).
More often it develops in the first hours (less often - days of the disease) with paroxysmal ventricular tachycardia, also with supraventricular tachycardia, paroxysmal atrial fibrillation and atrial flutter. The general condition of the patient is serious.
All clinical signs of shock are expressed:
Significant arterial hypotension;
Symptoms of peripheral circulatory failure;
Oligoanuria;
30% of patients develop severe acute left ventricular failure;
Complications: ventricular fibrillation, thromboembolism in vital organs;
Relapses of paroxysmal tachycardias, expansion of the necrosis zone, development of cardiogenic shock.
2. Bradysystolic (bradyarrhythmic variant of cardiogenic shock).
Develops with complete atrioventricular block with conduction 2:1, 3:1, slow idioventricular and nodal rhythms, Frederick's syndrome (a combination of complete atrioventricular block with atrial fibrillation). Bradysystolic cardiogenic shock is observed in the first hours of the development of extensive and transmural myocardial infarction.
The course of shock is severe;
Mortality reaches 60% or more;
The causes of death are severe left ventricular failure, sudden cardiac asystole, ventricular fibrillation.
There are 3 degrees of severity of cardiogenic shock depending on the severity of clinical manifestations, hemodynamic parameters, and response to measures taken:
1. First degree:
Duration no more than 3-5 hours;
Systolic blood pressure 90 -81 mm Hg;
Pulse blood pressure 30-25 mm Hg;
Symptoms of shock are mild;
Heart failure is absent or mild;
Rapid sustained pressor response to therapeutic measures.
2. Second degree:
Duration 5-10 hours;
Systolic blood pressure 80-61 mm Hg;
Pulse blood pressure 20-15 mm Hg;
Symptoms of shock are pronounced;
Severe symptoms of acute left ventricular failure;
Slow, unstable pressor response to therapeutic measures.
3. Third degree:
More than 10 hours;
Systolic blood pressure less than 60 mm Hg, may fall to 0;
Pulse blood pressure less than 15 mmHg;
The course of shock is extremely severe;
Severe heart failure, severe pulmonary edema;
There is no pressor reaction to treatment, an areactive state develops.
List of main diagnostic measures:
1. ECG diagnostics.
List of additional diagnostic measures:
1. Measurement of the CVP level (for resuscitation teams).
Treatment abroad
Get treatment in Korea, Israel, Germany, USA
Get advice on medical tourism
Treatment
Tactics of medical care:
1. For reflex shock, the main treatment measure is quick and complete pain relief.
2. In case of arrhythmic shock, cardioversion or cardiac pacing is performed for health reasons.
3. For shock associated with myocardial rupture, only emergency surgical intervention is effective.
Treatment program for cardiogenic shock:
1.General activities:
1.1. Anesthesia.
1.2. Oxygen therapy.
1.3. Thrombolytic therapy.
1.4. Heart rate correction, hemodynamic monitoring.
2. Intravenous fluid administration.
3. Decrease in peripheral vascular resistance.
4. Increased myocardial contractility.
5. Intra-aortic balloon counterpulsation.
6. Surgical treatment.
Emergency treatment is carried out in stages, quickly moving to the next stage if the previous one is ineffective.
1. In the absence of pronounced congestion in the lungs:
Lay the patient down with the lower limbs elevated at an angle of 20º;
Carry out oxygen therapy;
Pain relief: morphine 2-5 mg IV, again after 30 minutes. or fentanyl 1-2 ml 0.005% (0.05 - 0.1 mg with droperidol 2 ml 0.25% IV diazepam 3-5 mg for psychomotor agitation;
Thrombolytics according to indications;
Heparin 5000 units intravenously;
Correct heart rate (paroxysmal tachycardia with heart rate more than 150 per minute is an absolute indication for cardioversion).
2. In the absence of pronounced congestion in the lungs and signs of increased central venous pressure:
200 ml 0.9; sodium chloride intravenously over 10 minutes, monitoring blood pressure, central venous pressure, respiratory rate, auscultatory picture of the lungs and heart;
In the absence of signs of transfusion hypervolemia (CVP below 15 cm H2O), continue infusion therapy using rheopolyglucin or dextran or 5% glucose solution at a rate of up to 500 ml/hour, monitoring the readings every 15 minutes;
If blood pressure cannot be stabilized quickly, proceed to the next stage.
3. If IV fluid administration is contraindicated or unsuccessful, peripheral vasodilators - sodium nitroprusside - are administered at a rate of 15-400 mcg/min. or isoket 10 mg in an infusion solution intravenously.
4. Inject dopamine(dopamine) 200 mg in 400 ml of 5% glucose solution as an intravenous infusion, increasing the infusion rate from 5 mcg/kg/min. until the minimum sufficient blood pressure is achieved;
There is no effect - additionally prescribe norepinephrine hydrotartrate 4 mg in 200 ml of 5% glucose solution intravenously, increasing the infusion rate from 5 mcg/min. until the minimum sufficient blood pressure is achieved.
3.*Diazepam 0.5% 2 ml, amp.
5.*Isosorbide dinitrate (isoket) 0.1% 10 ml, amp.
6.*Norepinephrine hydrotartrate 0.2% 1 ml, amp.
Indicators of the effectiveness of medical care:
1. Relief of pain syndrome.
2. Relief of rhythm and conduction disturbances.
3. Relief of acute left ventricular failure.
4. Stabilization of hemodynamics.
Information
Sources and literature
- Protocols for diagnosis and treatment of diseases of the Ministry of Health of the Republic of Kazakhstan (Order No. 764 of December 28, 2007)
- 1. Diagnosis of diseases of internal organs, volume 3, vol. 6, A.N. Okorokov, Moscow, 2002, 2. Recommendations for the provision of emergency medical care in the Russian Federation, 2nd edition, ed. A.G. Miroshnichenko, V.V. Ruksina, St. Petersburg, 2006 3. Advanced Cardiac Life Support, AAC, 1999, translated from English, E.K. Sisengaliev, Almaty PDF created with pdfFactory Pro trial version www.pdffactory.com 4. Birtanov E.A., Novikov S.V., Akshalova D.Z. Development of clinical guidelines and diagnostic and treatment protocols taking into account modern requirements. Methodological recommendations. Almaty, 2006, 44 p. 5. Order of the Minister of Health of the Republic of Kazakhstan dated December 22, 2004 No. 883 “On approval of the List of essential (vital) medicines.” 6. Order of the Minister of Health of the Republic of Kazakhstan dated November 30, 2005 No. 542 “On introducing amendments and additions to the order of the Ministry of Health of the Republic of Kazakhstan dated December 7, 2004 No. 854 “On approval of the Instructions for the formation of the List of essential (vital) medicines.”
Information
Head of the Department of Emergency and Emergency Medical Care, Internal Medicine No. 2, Kazakh National Medical University named after. S.D. Asfendiyarova - Doctor of Medical Sciences, Professor Turlanov K.M.
Employees of the Department of Ambulance and Emergency Medical Care, Internal Medicine No. 2 of the Kazakh National Medical University named after. S.D. Asfendiyarova: candidate of medical sciences, associate professor Vodnev V.P.; candidate of medical sciences, associate professor Dyusembayev B.K.; Candidate of Medical Sciences, Associate Professor Akhmetova G.D.; candidate of medical sciences, associate professor Bedelbaeva G.G.; Almukhambetov M.K.; Lozhkin A.A.; Madenov N.N.
Head of the Department of Emergency Medicine of the Almaty State Institute for Advanced Medical Studies - Candidate of Medical Sciences, Associate Professor Rakhimbaev R.S.
Employees of the Department of Emergency Medicine of the Almaty State Institute for Advanced Medical Studies: Candidate of Medical Sciences, Associate Professor Silachev Yu.Ya.; Volkova N.V.; Khairulin R.Z.; Sedenko V.A.
Attached files
Attention!
- By self-medicating, you can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" cannot and should not replace a face-to-face consultation with a doctor. Be sure to contact a medical facility if you have any illnesses or symptoms that concern you.
- The choice of medications and their dosage must be discussed with a specialist. Only a doctor can prescribe the right medicine and its dosage, taking into account the disease and condition of the patient’s body.
- The MedElement website and mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Directory" are exclusively information and reference resources. The information posted on this site should not be used to unauthorizedly change doctor's orders.
- The editors of MedElement are not responsible for any personal injury or property damage resulting from the use of this site.
Cardiogenic shock is a pathological process when the contractile function of the left ventricle fails, the blood supply to tissues and internal organs deteriorates, which often ends in human death.
It should be understood that cardiogenic shock is not an independent disease, and the cause of the anomaly may be another disease, condition, or other life-threatening pathological processes.
The condition is extremely life-threatening: if proper first aid is not provided, death occurs. Unfortunately, in some cases, even assistance from qualified doctors is not enough: statistics are such that in 90% of cases biological death occurs.
Complications that occur regardless of the stage of development of the condition can lead to serious consequences: the blood circulation of all organs and tissues is disrupted, the brain, acute and in the digestive organs can develop, and so on.
According to the International Classification of Diseases, Tenth Revision, the condition is located in the section “Symptoms, signs and abnormalities that are not classified elsewhere.” The ICD-10 code is R57.0.
Etiology
In most cases, cardiogenic shock develops during myocardial infarction as a complication. But there are other etiological factors for the development of the anomaly. The causes of cardiogenic shock are as follows:
- complication after;
- poisoning with cardiac substances;
- pulmonary artery;
- intracardiac bleeding or effusion;
- poor pumping function of the heart;
- heavy;
- acute valvular insufficiency;
- hypertrophic;
- rupture of the interventricular septum;
- traumatic or inflammatory damage to the pericardial sac.
Any condition is extremely life-threatening, so if you have a diagnosis, you need to carefully follow the doctor’s recommendations, and if you feel unwell, urgently seek medical help.
Pathogenesis
The pathogenesis of cardiogenic shock is as follows:
- as a result of certain etiological factors, a sharp decrease in cardiac output occurs;
- the heart can no longer fully provide blood supply to the body, including the brain;
- acidosis also develops;
- the pathological process may be aggravated by ventricular fibrillation;
- asystole and respiratory arrest occur;
- If resuscitation measures do not give the desired result, the patient dies.
The problem develops very quickly, so there is virtually no time for treatment.
Classification
Heart rate, blood pressure, clinical signs and duration of the abnormal condition define three degrees of cardiogenic shock. There are several other clinical forms of the pathological process.
Types of cardiogenic shock:
- reflex cardiogenic shock - easily relieved, characterized by severe pain;
- arrhythmic shock - associated with or caused by low cardiac output;
- true cardiogenic shock - the classification regards such cardiogenic shock as the most dangerous (death occurs in almost 100%, because pathogenesis leads to irreversible changes that are incompatible with life);
- areactive - according to the development mechanism, it is actually an analogue of true cardiogenic shock, but the pathogenetic factors are more pronounced;
- cardiogenic shock due to myocardial rupture - a sharp drop in blood pressure, cardiac tamponade as a result of previous pathological processes.
Regardless of what form of the pathological process is present, the patient must urgently receive first aid for cardiogenic shock.
Symptoms
Clinical signs of cardiogenic shock are similar to those of a heart attack and similar pathological processes. The anomaly cannot be asymptomatic.
Symptoms of cardiogenic shock:
- weak, thready pulse;
- a sharp decrease in blood pressure;
- decrease in the daily amount of urine excreted - less than 20 ml/hour;
- lethargy of a person, in some cases a coma occurs;
- pale skin, sometimes acrocyanosis occurs;
- pulmonary edema with corresponding symptoms;
- decreased skin temperature;
- shallow, wheezing breathing;
- increased sweating, sticky sweat;
- muffled heart sounds are heard;
- sharp pain in the chest, which radiates to the area of the shoulder blades and arms;
- if the patient is conscious, there is panic, anxiety, and possibly a state of delirium.
Failure to receive immediate treatment for symptoms of cardiogenic shock will inevitably lead to death.
Diagnostics
The symptoms of cardiogenic shock are pronounced, so there are no problems with making a diagnosis. First of all, resuscitation measures are carried out to stabilize the person’s condition, and only then diagnostics are carried out.
Diagnosis of cardiogenic shock includes the following procedures:
- chest x-ray;
- angiography;
- echocardiography;
- electrocardiography
- biochemical blood test;
- arterial blood sampling for analysis of gas composition.
Diagnostic criteria for cardiogenic shock are taken into account:
- heart sounds are muffled, a third tone can be detected;
- kidney function - diuresis or anuria;
- pulse - thread-like, small filling;
- blood pressure indicators are reduced to a critical minimum;
- breathing - shallow, labored, with a high rise of the chest;
- pain - sharp, throughout the chest, radiating to the back, neck and arms;
- human consciousness - semi-delirium, loss of consciousness, coma.
Based on the results of diagnostic measures, treatment tactics for cardiogenic shock are selected - medications are selected and general recommendations are drawn up.
Treatment
The chances of recovery can be increased only if the patient receives timely and correct pre-medical care. Along with these activities, you should call an emergency medical team and clearly describe the symptoms.
Provide emergency care for cardiogenic shock according to the following algorithm:
- lay the person on a hard, flat surface and raise their legs;
- unbutton the collar and belt of the trousers;
- provide access to fresh air, if this is a room;
- if the patient is conscious, give a Nitroglycerin tablet;
- if there are visible signs of cardiac arrest, begin indirect massage.
The ambulance team can carry out the following life-saving measures:
- injections of painkillers - a drug from the group of nitrates or narcotic analgesics;
- with - fast-acting diuretics;
- the drug "Dopamine" and adrenaline for cardiogenic shock - if cardiac arrest occurs;
- to stimulate cardiac activity, the drug “Dobutamine” is administered in a diluted form;
- providing oxygen using a cylinder or pillow.

Intensive care for cardiogenic shock significantly increases the chances that a person will not die. The algorithm for providing assistance is approximate, since the actions of doctors will depend on the patient’s condition.
Treatment of cardiogenic shock due to myocardial infarction and other etiological factors directly in a medical institution may include the following measures:
- to carry out infusion therapy, a catheter is inserted into the subclavian vein;
- the causes of the development of cardiogenic shock are determined diagnostically and a drug is selected to eliminate them;
- if the patient is unconscious, the person is transferred to artificial ventilation;
- installation of a catheter in the bladder to control the amount of urine produced;
- drugs are administered to increase blood pressure;
- injections of drugs of the catecholamine group (“Dopamine”, “Adrenaline”) if cardiac arrest occurs;
- To restore the impaired coagulating properties of blood, Heparin is administered.
In the process of carrying out measures to stabilize the condition, drugs with the following spectrum of action can be used:
- analgesics;
- vasopressors;
- cardiac glycosides;
- phosphodiesterase inhibitors.
It is impossible to independently give the patient hemodynamic drugs and other drugs (with the exception of Nitroglycerin).
If infusion therapy for cardiogenic shock does not produce the desired result, a decision regarding surgical intervention is urgently made.
In this case, coronary angioplasty can be performed with further installation of a stent and a solution to the issue of bypass surgery. The most effective method for such a diagnosis could be an emergency heart transplant, but this is practically impossible.
Unfortunately, in most cases, cardiogenic shock leads to death. But providing emergency care for cardiogenic shock still gives a person a chance to survive. There are no preventive measures.
Is everything in the article correct from a medical point of view?
Answer only if you have proven medical knowledge
Treatment of cardiogenic shock. Cardiogenic shock is a serious complication of myocardial infarction, the mortality rate of which reaches 80% or more. Its treatment is a complex task and includes a set of measures aimed at protecting the ischemic myocardium and restoring its functions, eliminating microcirculatory disorders, and compensating for impaired functions of parenchymal organs. The effectiveness of treatment measures largely depends on the time of their initiation. Early treatment of cardiogenic shock is the key to success. The main task that needs to be solved as soon as possible is stabilization of blood pressure at a level that ensures adequate perfusion of vital organs (90-100 mm).
The sequence of treatment measures for cardiogenic shock:
1. Relief of pain syndrome. Since the intense pain syndrome that occurs during myocardial infarction is one of the reasons for the decrease in blood pressure, all measures must be taken to quickly and completely relieve it. The most effective use of neuroleptanalgesia.
2. Normalization of heart rhythm. Stabilization of hemodynamics is impossible without eliminating cardiac arrhythmias, since an acute attack of tachycardia or bradycardia in conditions of myocardial ischemia leads to a sharp decrease in stroke and cardiac output. The most effective and safe way to stop tachycardia with low blood pressure is electrical pulse therapy. If the situation allows for drug treatment, the choice of antiarrhythmic drug depends on the type of arrhythmia. For bradycardia, which is usually caused by acute atrioventricular block, almost the only effective remedy is endocardial pacing. Injections of atropine sulfate most often do not provide a significant and lasting effect.
3. Strengthening the inotronic function of the myocardium. If, after eliminating the pain syndrome and normalizing the frequency of ventricular contraction, blood pressure does not stabilize, then this indicates the development of true cardiogenic shock. In this situation, it is necessary to increase the contractile activity of the left ventricle, stimulating the remaining viable myocardium. For this purpose, sympathomimetic amines are used: dopamine (Dopamine) and dobutamine (Dobutrex), which selectively act on beta-1 adrenergic receptors of the heart. Dopamine is administered intravenously. To do this, 200 mg (1 ampoule) of the drug is diluted in 250-500 ml of 5% glucose solution. The dose in each specific case is selected empirically depending on the dynamics of blood pressure. Usually start with 2-5 mcg/kg per 1 min (5-10 drops per 1 min), gradually increasing the rate of administration until the systolic blood pressure stabilizes at 100-110 mm Dobutrex is available in 25 ml bottles containing 250 mg of dobutamine hydrochloride in lyophilized form. Before use, the dry substance in the bottle is dissolved by adding 10 ml of solvent, and then diluted in 250-500 ml of 5% glucose solution. Intravenous infusion is started with a dose of 5 mcg/kg per 1 minute, increasing it until a clinical effect appears. The optimal rate of administration is selected individually. It rarely exceeds 40 mcg/kg per minute; the effect of the drug begins 1-2 minutes after administration and ceases very quickly after its completion due to its short (2 min) half-life.
4. Nonspecific anti-shock measures. Simultaneously with the administration of sympathomimetic amines, the following drugs are used to influence various parts of the pathogenesis of shock:
1. Glucocorticoids: prednisolone - 100-120 mg intravenously;
2. Heparin - 10,000 units intravenously;
3. Sodium bicarbonate - 100-120 ml of 7.5% solution;
4. Reopoliglucin - 200-400 ml, if the administration of large quantities of liquid is not contraindicated (for example, when shock is combined with pulmonary edema); In addition, oxygen inhalations are carried out.
Despite the development of new approaches to the treatment of cardiogenic shock, the mortality rate for this complication of myocardial infarction ranges from 85 to 100%. Therefore, the best “treatment” for shock is its prevention, which consists of quickly and completely relieving pain, heart rhythm disturbances and limiting the area of infarction.









